








APA
ISO 690-2
Harvard
Haga clic en un formato de citación
Stakeholder Evaluation of Health and Wellbeing Outcomes of Inclusive Public Space Interventions Delivered by the IN-HABIT Project*
Evaluación de los actores involucrados sobre los resultados en salud y bienestar de las intervenciones en espacios públicos inclusivos implementadas por el proyecto IN-HABIT
Avaliação dos atores envolvidos sobre os resultados em saúde e bem-estar das intervenções em espaços públicos inclusivos implementadas pelo projeto IN-HABIT
Yuliia Hodnieva ![]() , Katarína Melichová
, Katarína Melichová ![]() , Soňa Bellérová
, Soňa Bellérová ![]() , Jana Kuffová Popovicsová
, Jana Kuffová Popovicsová ![]()
Stakeholder Evaluation of Health and Wellbeing Outcomes of Inclusive Public Space Interventions Delivered by the IN-HABIT Project*
Cuadernos de Vivienda y Urbanismo, vol. 18, 2025
Pontificia Universidad Javeriana
Yuliia Hodnieva a xhodnieva@uniag.sk
Slovak University of Agriculture in Nitra, Eslovaquia
Katarína Melichová
Slovak University of Agriculture in Nitra, Eslovaquia
Soňa Bellérová
Slovak University of Agriculture in Nitra, Eslovaquia
Jana Kuffová Popovicsová
Slovak University of Agriculture in Nitra, Eslovaquia
Received: 05 february 2025
Accepted: 20 may 2025
Published: 09 september 2025
Abstract: The article reports on the evaluation of the health and well-being outcomes of inclusive public space interventions co-designed, co-deployed, and co-managed within the IN-HABIT project in Nitra, Slovakia. Based on data from a questionnaire survey, the research highlights variations in perceived benefits across diverse social groups. Psychological well-being improved most among marginalised communities, while social cohesion and spatial satisfaction were significant across all target groups. The most substantial benefits were reported not merely from experiencing improved public spaces but from active participation in their design, implementation, and governance. These findings suggest that genuinely inclusive and impactful urban development should prioritise meaningful community participation, ensuring that interventions reflect the needs, aspirations, and lived experiences of diverse populations. By embedding participatory approaches into urban planning, cities can foster more equitable, resilient, and health-promoting environments.
Keywords:Co-Design, Health and Well-Being, Inclusive Urban Development, Participatory Urban Planning, Public Space Interventions, Vulnerable Communities.
Resumen: El artículo hace referencia a la evaluación de los resultados en salud y bienestar de las intervenciones en espacios públicos inclusivos, co-diseñadas, co-implementadas y co-gestionadas dentro del proyecto IN-HABIT en Nitra, Eslovaquia, basado en los datos de una encuesta por cuestionario; la investigación destaca variaciones en los beneficios percibidos entre diferentes grupos sociales. El bienestar psicológico mejoró principalmente entre las comunidades marginadas, mientras que la cohesión social y la satisfacción espacial fueron significativas en todos los grupos objetivo. Los mayores beneficios no se reportaron únicamente por la experiencia de espacios públicos mejorados, sino por la participación activa en su diseño, implementación y gestión. Estos hallazgos sugieren que un desarrollo urbano verdaderamente inclusivo y efectivo debe priorizar la participación significativa de la comunidad, asegurando que las intervenciones reflejen las necesidades, aspiraciones y experiencias vividas de diversas poblaciones. Al integrar enfoques participativos en la planificación urbana, las ciudades pueden fomentar entornos más equitativos, resilientes y saludables.
Palabras clave: codiseño, desarrollo urbano inclusivo, espacios públicos inclusivos, participación urbana participativa, salud y bienestar, comunidades vulnerables.
Resumo: O artigo apresenta a avaliação dos resultados em saúde e bem-estar das intervenções em espaços públicos inclusivos, co-desenhadas, co-implementadas e co-gerenciadas no âmbito do projeto IN-HABIT em Nitra, Eslováquia. Com base em dados de uma pesquisa por questionário, a pesquisa destaca variações nos benefícios percebidos entre diferentes grupos sociais. O bem-estar psicológico melhorou principalmente entre comunidades marginalizadas, enquanto a coesão social e a satisfação espacial foram significativas em todos os grupos-alvo. Os maiores benefícios não foram apenas a experiência de espaços públicos melhorados, mas a participação ativa no seu design, implementação e gestão. Esses achados sugerem que um desenvolvimento urbano verdadeiramente inclusivo e eficaz deve priorizar a participação significativa da comunidade, garantindo que as intervenções reflitam as necessidades, aspirações e experiências vividas por diversas populações. Ao incorporar abordagens participativas no planejamento urbano, as cidades podem promover ambientes mais equitativos, resilientes e saudáveis.
Palavras-chave: co-design, saúde e bem-estar, desenvolvimento urbano inclusivo, planejamento urbano participativo, intervenções em espaços públicos, comunidades vulneráveis.
Introduction
Inclusive public spaces play a fundamental role in urban health and well-being. Cities increasingly adopt innovative urban strategies to enhance quality of life and social inclusion (Romanelli, 2022). Successful models from European and Australian cities demonstrate how urbanization can drive inclusivity through adaptable housing and public space solutions (Ксендзук et al., 2023). Urban strategies emphasizing flexibility and connectivity improve the well-being of diverse populations, including migrants (Maruniak et al., 2021). Thoughtful urban design fosters physical activity, reduces stress, and enhances mental health, while poorly planned spaces contribute to social isolation (Salsabila & Navitas, 2024).
Aligning urban planning with global priorities, including the UN Sustainable Development Goals (SDGs) and European urban policies, is critical for sustainable and inclusive growth. Urban regeneration initiatives, such as Madrid’s Nuevo Norte, showcase how SDG-aligned projects improve sustainability while addressing social and economic needs (Álvarez-Melcón et al., 2024). However, evaluating the differential impacts of these interventions on diverse groups, including migrants, ethnic minorities, LGBTQI+ individuals, and the elderly, remains a crucial challenge (Cassarino et al., 2021; Peters, 2010). Understanding how different populations experience and benefit from inclusive public spaces is essential for designing equitable urban solutions (Mitrašinović & Mehta, 2021; Rishbeth, 2001). Particularly, assessing the health and well-being outcomes of such interventions in underrepresented communities requires more comprehensive approaches (Cassarino et al., 2021). While urban green spaces promote social cohesion, assessing their effectiveness in that respect requires participatory research with collaboration between researchers, policymakers, and communities (Jennings et al., 2024). Engaging communities in design and evaluation ensures more accessible and effective interventions (Anderson et al., 2017).
Gaps persist in understanding how participation in the design, interventions and maintenance of urban spaces impacts health and well-being. Despite growing interest in participatory planning, comprehensive assessment frameworks remain limited (Jian, 2021). Research lacks clarity on how collaborative urban interventions affect marginalised groups (Agarwala et al., 2014). While inclusive spaces aim to enhance social integration, empirical evidence on reducing health inequalities is scarce (Marmot & Allen, 2014). The interaction of social, environmental, and economic factors further complicates evaluation (Braubach et al., 2015). There is a need for the development of robust methodologies to quantify participatory urban approaches to promoting health and well-being and support evidence-based policymaking (Keating, 2016). Inclusive public spaces, integrated into urban policies, enhance community health, resilience, and equity.
The IN-HABIT project exemplifies integrating inclusive health and well-being aspects into urban planning through inclusive public space interventions. This EU-funded initiative focuses on marginalised groups, reducing health disparities in access to public, especially green public spaces and fostering community engagement. By collaborating with urban planners, policymakers, and local communities, the project advances accessibility, sustainability, and equitable development while demonstrating the role of participation in creating sustainable, people-centred cities. The case study presented in this article aims to address the current gaps in understanding how different social groups benefit from co-created inclusive public spaces. The project introduces the CO-CO-CO methodology – co-design, co-deployment, and co-management of innovative solutions mostly targeting green public spaces in four European small and medium-sized cities (Mac Fadden et al., 2024). This research focuses on one pilot city (Nitra, Slovakia) and explores the key health and well-being outcomes of inclusive public space interventions, as well as how different target groups perceive their benefits.
Theoretical Background
Inclusive Urban Development
Issues of inclusiveness are prominent today in both urban theory and international urban development policy (Bunnell, 2019). David Harvey’s The Right to the City (Harvey, 1973) emphasises the need for equitable access to urban opportunities, advocating for participatory governance in urban decision-making. Edward Soja’s Seeking Spatial Justice (Soja, 2010) builds upon this by highlighting how spatial inequalities exacerbate social and economic marginalisation. Both authors argue that urban spaces reflect and reinforce socioeconomic inequalities, making inclusive urban development necessary for social justice. Medayese et al. (2020) identified several studies analysing parameters and indicators essential for ensuring inclusive urban development that accommodates the needs of all population groups. They explored the intricate relationship between inclusive physical development and residents’ life expectations, various dimensions of inclusivity, its definitions, measurement scales, and appraisal methodologies (Medayese et al., 2020).
Inclusive urban development emphasises creating public spaces that cater to diverse populations, including children, low-income individuals, women, and people with disabilities (Ahmimed, 2018; Haider, 2007). Inclusivity in urban theory has evolved to incorporate experiences from cities beyond Western Europe and North America, challenging traditional urban studies (Bunnell, 2019, p. 89). Assessing public space inclusivity requires consideration of multiple factors, including spatial distribution, facilities, safety, and user categories, while the approach involves participatory planning, intergenerational perspectives, and innovative technology integration to enhance accessibility and user satisfaction (Itair et al., 2023). Recent studies have highlighted the relationship between inclusivity and physical development, emphasising the need to address all aspects of human composition in urban planning (Medayese et al., 2020, p. 24).
Co-design and co-management approaches are instrumental in fostering community growth, ownership and engagement in various contexts. These approaches uplift communities by recognising and mobilising existing assets, such as people’s skills, knowledge, and local resources, to drive collective improvements (Lam et al., 2017). Co-design and co-production serve as powerful approaches to uncover and mobilise existing assets within a community by fostering collaboration, shared ownership, and local engagement (Robert et al., 2022). Thomas et al. (2021) found that these approaches can lead to positive well-being outcomes and more user-centred services. However, their effective implementation requires considering enablers and constraints such as social capital, stakeholder attributes, and research design, while the lack of impact evaluation makes understanding how these methods compare to more traditional participatory approaches difficult (Nguyen et al., 2024). In this respect, collaboration with an experienced team of researchers who are well-versed in community settings and skilled in fostering respectful and meaningful engagement is crucial (Khan et al., 2024, p. 6).
Health and Well-Being Dimensions
Well-being is a multifaceted concept encompassing physical, mental, social, and environmental aspects, with each component interacting and varying in importance for individuals (Kiefer, 2008). It includes both subjective and objective dimensions, reflecting personal life experiences and comparisons with social norms (Sfeatcu et al., 2014), and is often measured through subjective life satisfaction, happiness, access to healthcare, educational attainment, employment status, and supportive relationships (Diener, 1984; Fleche et al., 2011; Haas, 1999). The social dimension of psychological well-being covers all social activities of the individual. It is an indicator of satisfaction or non-satisfaction with social needs and fulfilled roles, as well as areas of life that involve interpersonal interaction (Helliwell & Putnam, 2004). The degree of satisfaction with the quality of interpersonal relationships, social roles, and social status determines the social context of psychological well-being (Можаровська, 2021, p. 159).
A significant portion of the literature and empirical studies seeks to find relationships between subjective or perceived well-being and objective health outcomes (Howell et al., 2007). On the other hand, recent studies also focused on the spatial dimension of health and well-being. Fleuret & Prugneau (2015), when surveying students in university towns, found that their well-being is primarily influenced by spaces of capability, with their transitory presence in university towns affecting their perception of place. On the other hand, Ala-Mantila et al. (2018) suggest that the quality of life is higher in central pedestrian zones, while happiness peaks in car-oriented areas.
Finally, economic well-being is also a multifaceted concept on its own, influenced by various factors beyond traditional financial indicators. It encompasses income, employment, mental and physical health, education, social relationships, and government policies (Livingston et al., 2022, p. 1187). Researchers are developing more comprehensive measures of economic well-being that consider taxes, government transfers, corporate benefits, wealth changes, household production, and public expenditures (Wolff & Zacharias, 2003, p.51).
Recent research has focused on developing multidimensional well-being assessments that capture a more holistic view of the human experience beyond traditional indicators. These assessments incorporate various dimensions, such as subjective, psychological, social, and community well-being (Prilleltensky et al., 2015; Sarriera & Bedin, 2017). However, despite the growing interest in multidimensional well-being assessments, the field faces challenges due to inconsistent terminology, theories, and dimensions across different approaches (Schonhardt et al., 2023). Additionally, researchers have emphasised the importance of adapting these measures to local contexts (Collomb et al., 2012) and the importance of incorporating local flexibility into well-being frameworks (Agarwala et al., 2014).
Inclusive health and well-being are closely linked to the concept of “health justice”, which can be viewed as the pinnacle of health equity since systemic and structural barriers to health are removed (Benfer et al., 2021). Not all health and development disparities are indicators of inequity, but those that are clearly linked to social patterns that are theoretically and empirically consistent can be powerful diagnostic tools, and they are particularly important when they point to social factors that can be changed, particularly in comparison to other societies where such social disparities are much smaller (Keating, 2016).
The interconnectedness of health and well-being outcomes highlights how factors such as gender, ethnicity, age and other demographic characteristics influence people’s experiences of and access to resources (Sirgy, 2021). Research has shown that women, especially those from ethnic minority groups, often face compounded problems in accessing and experiencing health outcomes due to intersecting forms of discrimination (Crenshaw, 1989). In addition, age and ethnicity affect the prevalence of certain health conditions, with older people from marginalised ethnic groups having higher rates of chronic disease (National Institute on Aging, 2020). Understanding these intersections is critical to addressing health disparities and promoting equitable health outcomes for all demographic groups (Bauer, 2014).
Evaluation Frameworks
Assessing the impact of urban interventions requires different methodological approaches. Evaluating the impact of urban interventions requires the use of both quantitative and qualitative methods to provide a comprehensive picture of changes in the urban environment. Quantitative evaluations typically involve statistical methods to measure specific changes, such as morbidity, mortality, or economic well-being, following the implementation of urban change. For example, Duncan et al. (2012) use statistical models to estimate the health impacts of changes in the urban environment, while Anderson & Parker (2018) use econometric models to analyse the economic benefits of urban regeneration projects. Qualitative methods include interviews and focus groups to collect in-depth data on residents’ experiences. In addition, mixed methods that combine quantitative and qualitative approaches allow for a more detailed examination of change’s complex social and economic effects. For example, Marmot & Allen (2014) use a combination of statistical models and social interviews to assess health and well-being in the context of urban change, highlighting the importance of social determinants of health.
With respect to the aim of the study, the distinction between impact and outcome in well-being research is crucial. However, the terms “impact”, “outcome”, and “effect” are often used interchangeably. The impact is generally considered the longer-term effect of an outcome, and while outcomes are typically pre-defined and objectively measurable, impacts are more subjective and personal (Harding, 2014) and thus require mixed-method approaches to evaluate (Larson et al., 2018).
On the other hand, albeit in another field of study, Belcher et al. (2018) propose a new framework for defining and distinguishing the terms “outcome” and “impact” based on the “kind of change” rather than the degree or temporal nature of change. They modelled “impact” as a “results chain” or “results web” with three main kinds of results: outputs, outcomes, and realised benefits as a “series of causally interrelated steps”. Franks et al. (2011) focus on another aspect of social impact assessment they deemed not to have been given sufficient attention. They posit that “cumulative impacts”, rather than individual impacts, are what communities actually experience. They conclude that “while cumulative impacts can be generated from the aggregation and interactions of the impacts resulting from a single intervention, in general, the term refers to the issues of assessment and management across multiple activities and actors in one area”. On the other side of this discussion is Kiefer (2008), who emphasises the need to explore how individuals define and conceptualise health and well-being “for themselves or other individuals from the same group of stakeholders”. To address some of these issues, Meringolo et al. (2019) proposed a Community Impact model for community-level interventions that is consistent with community psychology methodologies and the PAR (Participatory Action Research) approach. The model comprises six steps that are strictly connected to one another and pertain to “forming accountable groups and leadership, transferring knowledge, transforming “bad data” into useful data, providing added value to interventions, and increasing local partnerships to create a more effective narrative regarding the implemented process and its outcomes.”
Methodology
The case study presented in this article draws from the data collected during the impact assessment phase of the IN-HABIT project in Nitra, Slovakia. IN-HABIT is a Horizon 2020 initiative wherein, from 2020 to 2025, partner cities from 4 EU states (Spain, Italy, Latvia and Slovakia) experiment with innovative solutions, so-called VIS (visionary and integrated solutions), to boost the health and well-being of diverse local communities. Different cities focus on various combinations of social, nature-based, cultural and technological innovations, but their approach applies the same CO-CO-CO philosophy. The CO-CO-CO approach is relevant to health and well-being assessment because it involves active community participation in the design, implementation and management of initiatives. As Marmot et al. (2012) point out, it increases the sustainability of solutions that reflect the real needs of the population. Co-deployment involves coordination between different groups to ensure equal access to resources, which is essential to prevent social inequalities in access to health services, as highlighted by Evans et al. (2015). Co-management allows local communities to actively participate in the long-term management of resources, which positively impacts health and well-being. Bauer (2014) emphasises that such management helps to reduce barriers to access to services and builds trust among participants.
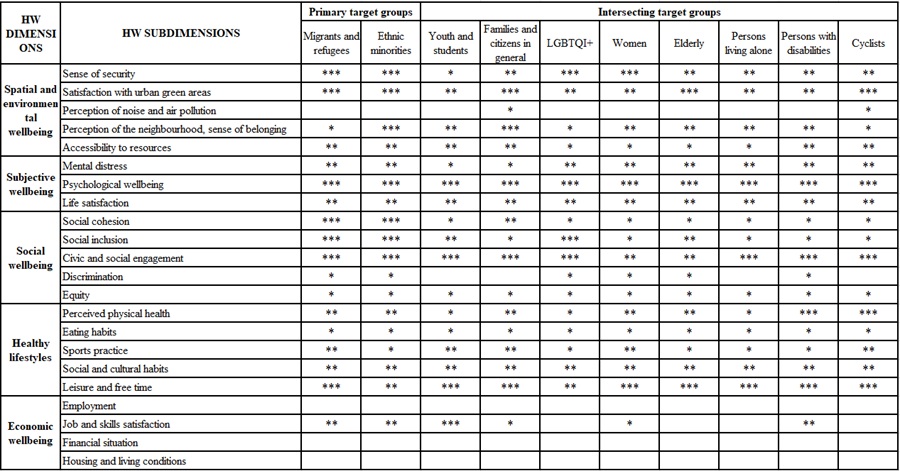
Concerning the IN-HABIT interventions in Nitra, both the VIS and their expected outcomes were co-designed with representatives of local communities. Primary target groups were migrants, ethnic minorities and refugees; however, to properly deconstruct the varying ways how our VIS contributed to persons and communities with different vulnerabilities and different stakes in the pilot area, another set of so-called “intersecting target groups” was identified (Table 1). By measuring and comparing the perceived contribution of solutions across these target groups, we seek to find the answer to the question of how inclusive the “inclusive health and well-being” generated by IN-HABIT interventions. Expected outcomes and/or impacts were identified individually for all target groups (also shown in Table 1) based on data collected during the co-design phase. When we refer to the “outcome” of VIS, we refer to the specific, immediate changes that result from that specific VIS for the individual involved, while the “impact” encompasses the broader and more significant reported or expected effects that those outcomes created or will amount to in the future, whether short-term or long-term, on the community (or target group) as a whole. The evaluation framework implemented in the case study was based on the health and well-being dimensions (HW) introduced by Mac Fadden et al. (2024).
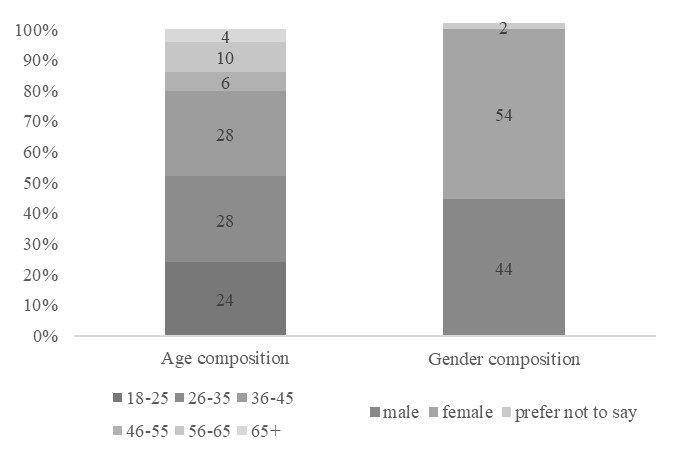
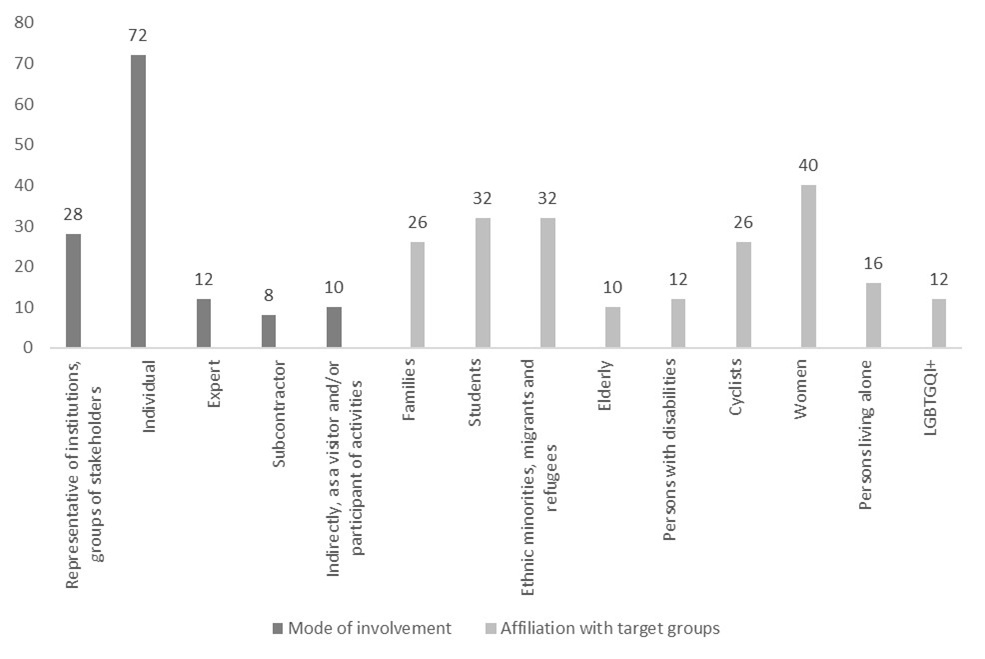
The assessment process relied on self-assessment and perception of the representatives of target groups and others involved. A semi-structured questionnaire was administered, where survey participants evaluated the overall impact of the CO-CO-CO process and the VIS themselves on the HW subdimension where outcomes were expected on a scale of 0 to 5, where 0 = I completely agree that [the process/VIS] contributed to [outcome]. Participants were chosen by purposive sampling: individuals involved either in the co-design or co-deployment phase or direct beneficiaries were deliberatively selected. A total of 50 respondents participated in this survey. Figure 1 illustrates their composition by demographic factors, and figure 2 shows their mode of involvement and affiliation with target groups. Individuals who participated in the IN-HABIT project were either individual target group representatives, experts, urban planners, and policymakers or institutional representatives of the target groups and other relevant stakeholders operating within the pilot area.
Results
This section of the article reports on the assessment of the health and well-being outcomes attributed to the process, and VIS generated through the IN-HABIT project by the survey participants. Figure 3 illustrates the distribution of average scores that survey participants awarded when asked about the contribution of all VIS and interventions to the 5 HW dimensions (for subjective wellbeing, we report life satisfaction and psychological wellbeing dimensions separately). The evaluation of individual HW indicators by the survey participants is depicted in figure 4. Here, we also compare their subjective evaluation of the contribution of the CO-CO-CO process versus the contribution of the VIS deployed to gain a better understanding of the IN-HABIT project and the outcomes in terms of 5 HW dimensions. It is important to note that in several instances, the co-design, co-deployment and co-management activities cannot be easily delineated, and many VIS were deployed together. For example, art residencies organised as VIS encompassed both the co-design activities carried out by the artist together with target groups and other visitors to the space where the installation was deployed, as well as the participatory creation of the installation itself. Similarly, with some workshops, small interventions were carried out during the co-design phase, while during the co-deployment phase of physical solutions, ad-hoc changes were made to the planned VIS. All the while, both individuals and organisations that co-manage the spaces in question were present and involved.
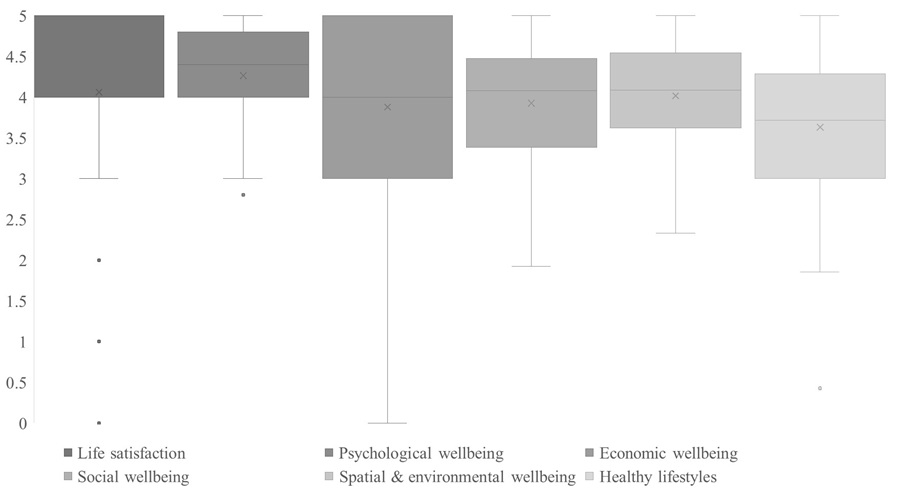
Figure 3 indicates that, overall, local stakeholders involved in different activities and interventions within the IN-HABIT project agree that developed and deployed VIS positively contributed to the 5 HW dimensions. However, we can also observe different intensities of contribution in different dimensions, as well as a certain degree of variability in the stakeholders’ opinions. On average, the highest score, also with the lowest degree of variability, was assigned by participants to the psychological well-being subdimension. When looking at the rating of individual adapted items of the WHO-5 scale used for the assessment (Figure 4), the strongest positive impact of VIS was felt in increased cheerfulness and good spirit, and even stronger in activity and vigorousness. On average, a similar degree of impact was assigned to the contribution of VIS to overall life satisfaction, although here, we see a higher degree of variability in participants’ evaluation, with several indicating that they do not agree that VIS contributed to this HW dimension at all.
The least positive evaluation by local stakeholders was found in terms of economic wellbeing: although the average score was 4, we also found the highest degree of disagreement between survey participants, with a portion of them not agreeing that IN-HABIT VIS contributed to economic wellbeing. It is pertinent to point out that economic wellbeing was the HW dimension that we least expected to contribute to, with the expected impact only in terms of satisfaction with skills and competencies, and also in a limited number of target groups.
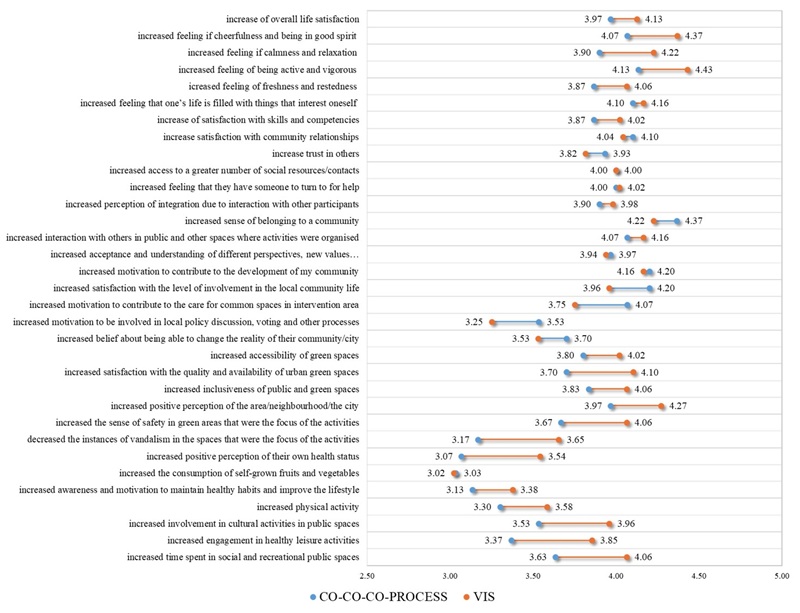
With average score of 4, subdimensions of social wellbeing and spatial and environmental wellbeing show comparable subjective positive changes as evaluated by local stakeholders, with a slightly higher consensus about outcomes in terms of spatial and environmental wellbeing. In terms of social wellbeing, social cohesion and social inclusion subdimensions were evaluated relatively similarly. Especially in case of social cohesion, specific indicators were scored very closely on average, with only slightly higher perceived change in satisfaction with relationships in the community, and slightly lower impact on trust in others. Very similar slight differences can be found in social inclusion indicators, with sense of belonging to a community scoring highest, and openness to diversity measured by increased acceptance and understanding of different perspectives scoring lowest in this subdimension. More significant differences in scoring were found in indicators of civic and social engagement subdimension. While the motivation to contribute to the development of their community was more positively affected by VIS deployed and their participation, this didn’t not translate to the same degree to their motivation to be involved in local policy discussion and other democratic processes, which they scored lower by almost an entire point.
However, when we compare individual average scores for social wellbeing indicators in figure 4, what we uncover is, that this is the subdimension where the process (meaning their involvement in the co-design, co-deployment and co-management) was perceived to have a stronger positive impact that the VIS themselves. This is true for all indicators of civic and social engagement, with the most notable contribution to motivation for democratic participation, engagement in caring for common spaces and their change-making attitudes. In terms of social cohesion and inclusion, their participation in the CO-CO-CO process more significantly contributed to their trust in others as well as their sense of belonging to the community. These findings underscore the importance of active participation and involvement in community processes as a driver of social well-being, suggesting that the sole experience of being engaged in shaping one’s environment can be more influential than the outcomes of the interventions. This highlights the value of inclusive, collaborative processes in strengthening social bonds and fostering a more cohesive and inclusive community fabric and demonstrates that while interventions can positively influence social well-being, the processes that involve individuals in meaningful ways can have an even greater impact.
The average contribution score to spatial and environmental wellbeing as perceived by local stakeholders reached 4 as well (Figure 3); however, if we analyse individual indicators separately (Figure 4), we also observe slight differences, most notably between the spatial wellbeing subdimension and perception of security. Spatial well-being indicators show slightly higher perceived positive change, especially an increase in positive perception of the area and increased satisfaction with the quality and availability of urban green spaces. On the other hand, the perceived impact on the perception of security was lower on average by half a point, with the frequency of vandalism being the one least affected by deployed VIS.
Of all HW dimensions, according to local stakeholders involved in the IN-HABIT project, the healthy lifestyles dimension was the least affected by deployed VIS or the CO-CO-CO process. The lowest perceived change happened in the consumption of self-grown fruits and vegetables and motivation to maintain healthy habits. On the other hand, local stakeholders reported that VIS contributed to their time spent in social and recreation public spaces, involvement in cultural activities in public spaces and their engagement in healthy leisure activities. Self-reported health status and physical activity were also less affected by VIS compared to other evaluated subdimensions.
With the aim of finding out how were the effects of visionary and integrated solutions deployed within the IN-HABIT project distributed between different target groups, we also compared the distribution of average scores within different HW dimensions (Figure 5) between those who indicated their affiliation to the given target groups and those participants who do not fall within said group. The analysis also compares average scores of individual evaluation indicators that were used to assess the 5 HW dimensions of select target groups (Figure 6).
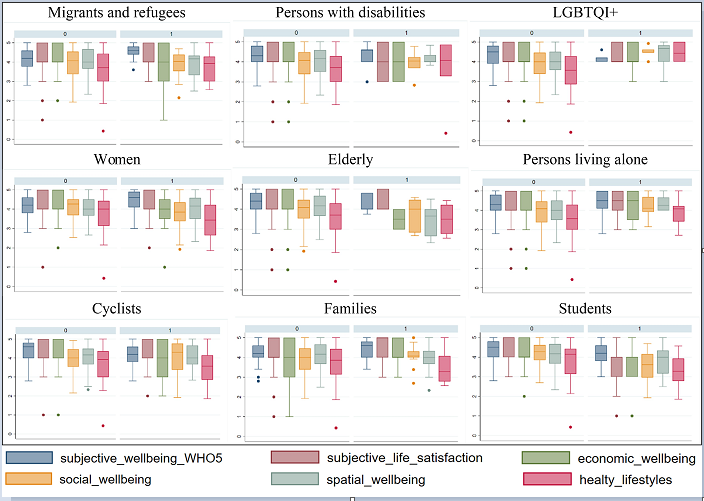
In the case of migrants and refugees participating in project activities, they show a higher positive effect of VIS on psychological well-being than the rest of the participants but the same level of effect on life satisfaction. They reported a comparable average effect on economic well-being, but with a markedly higher degree of variability, with a number of respondents stating a very low effect. In terms of healthy lifestyles, they report slightly higher scores of effect than the rest of the participants, as well as in terms of spatial wellbeing, although here we find a significant portion scoring lower than those without migrant background. The positive impact in the healthy lifestyles dimension lies mostly in the positive scoring of effects of VIS on their leisure and free time opportunities and cultural consumption; this, however, is not reflected in their perceived health status, which was scored lower than most other target groups (Figure 6). There appears to be little difference between the perceived effects of VIS on social well-being. In this dimension, they scored relatively high (Figure 6) on the effect of VIS on their sense of belonging and perception of integration due to interaction with others, as well as engagement in voluntary activities and openness to diversity. On the other hand, this did not affect their change-making attitudes and motivation for democratic participation.
Persons with disabilities report comparable effects on VIS with those without disabilities. However, we can observe non-agreement in this group regarding the effect on overall life satisfaction and economic well-being. Conversely, they mostly agree on a positive effect on social and spatial well-being. This target group felt, on average, a slightly higher effect of VIS on healthy lifestyles, specifically in individual indicators of leisure/free time and cultural consumption subdimensions (Figure 6). They also report a relatively higher effect on their physical activity, however, this does not translate into a significant impact on self-reported health status.
According to LGBTQI+ participants, the overall effect of VIS was higher on social and spatial well-being, as well as healthy lifestyles, when compared to heterosexual and cisgender participants. When analysing their average scoring of individual HW indicators (Figure 6), we observe that the most positive effects of VIS in this group were felt in terms of an increase in social resources and contacts, the feeling of having someone to turn to for help, perception of integration, openness to diversity and engagement in voluntary activities in case of social wellbeing. In the case of spatial wellbeing, they felt a considerable effect on the sense of safety in green areas and their inclusiveness and positive perception of the area. In terms of healthy habits, they also reported higher than average effects on healthy leisure opportunities and time spent outdoors, but contrary to most other target groups, they also reported positive effects on self-grown fruit and vegetable consumption and motivation towards healthy habits.
Women have assessed effects on their subjective psychological well-being and spatial well-being higher than the rest of the participants, while the perceived effect of VIS on their economic well-being, social well-being and healthy lifestyle dimensions is comparatively lower. They were more pessimistic than the rest of the participants in evaluating the impact of VIS on their change-making attitudes but scored a higher impact of VIS on the accessibility of local resources, specifically green spaces and on positive perception of the neighbourhood than the rest of the participants. We can also see that the effects were not perceived as strongly by elderly participants, especially in terms of economic well-being and spatial well-being. When we analyse the average scores of individual indicators (Figure 6), we can observe that this is the target group that scored a number of evaluation indicators the lowest, namely: the impacts on jobs and skill satisfaction, engagement in caring for common spaces and local community activities, satisfaction with urban green areas, their inclusiveness and positive perception of the neighbourhood, and in terms of healthy lifestyles they report lower effect on their physical activity and perceived health status. Conversely, persons living alone felt the impact of VIS more strongly than their counterparts, most notably in spatial and social well-being dimensions, as well as healthy lifestyles dimension. According to this group, the greatest positive impact of VIS was felt in job and skill satisfaction, satisfaction with personal relationships in the community, and increased trust in others. They also reported a higher degree of social inclusion, particularly openness to diversity, an increase in contact with others in public spaces, and increased motivation to care for said common public spaces. Strong self-reported effects can also be seen in their satisfaction with urban green areas, their inclusiveness, and the accessibility of local resources. They also report higher physical activity practice as a result of their involvement in IN-HABIT. With participants representing the target group “families”, we can observe the opposite tendency in several dimensions, namely the lower average score in spatial well-being and healthy lifestyles. However, their perceived effects on psychological well-being were, on average, higher than the rest of the participants.
Since a lot of the interventions were planned and deployed around a cyclotraffic corridor and bike path connecting the locations of interest, we also included a specific target group – cyclists. This group reported a lower impact of VIS on their psychological well-being than non-cyclists, as well as a lower effect on economic well-being and healthy lifestyles. On the other hand, they rated the effect on social well-being more strongly on average but showed greater variability of opinions. This higher effect was mostly driven by the perceived strong impact of VIS on increased contacts with others in public spaces, a sense of belonging to a community and engagement in local community activities. While the spatial well-being dimensions in this target group also show variability in perceived impact, most of them strongly agree that VIS contributed to the accessibility of green spaces, satisfaction in urban green areas and positive perception of the area.
The students involved in the IN-HABIT VIS scored their impact on all HW dimensions on average lower than the rest of the participants, with the exception of spatial wellbeing. They felt that the lowest effect of their involvement in VIS was reached in terms of an increase in trust in others, their social network support, and also, surprisingly, in job and skill satisfaction. This directly contradicts their verbal assessment of the VIS they were involved in.

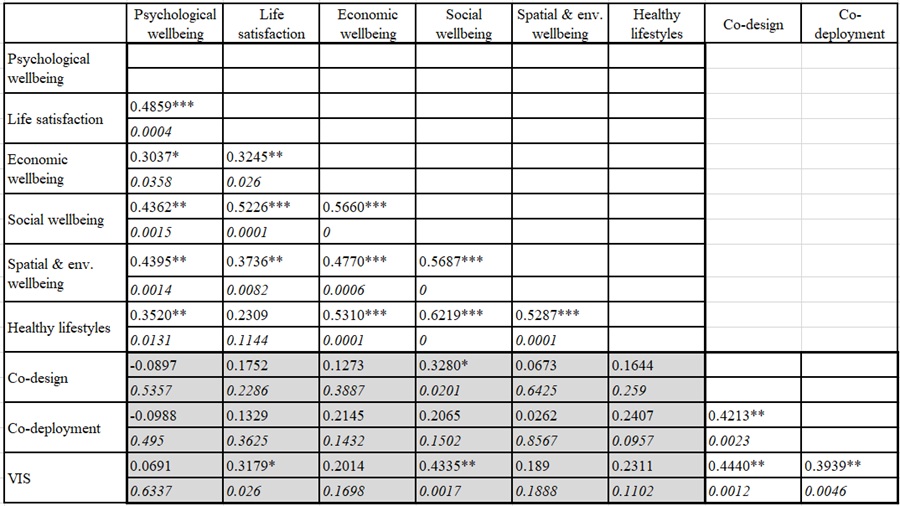
To find out whether the frequency or intensity of participants’ involvement in the IN-HABIT process and VIS led to higher perceived benefits from those solutions, we conducted a simple correlation analysis (Table 2). Intensity of involvement was quantified as a sum of activities that a particular survey participant participated in within three phases: the co-design, co-deployment activities and VIS themselves. What the correlation analysis suggests is that the strongest impact of more frequent interaction with deployed solutions leads to greater perceived benefits in terms of social well-being (coef.: 0.4335, p-value: 0.0017) and to a lesser degree to increase in overall life satisfaction (coef.: 0.3179, p-value: 0.026). The more frequent involvement in the co-design process also led to a statistically significant higher reported impact on social well-being (coef.: 0.3280, p-value: 0.0201). This further supports the respondents’ self-reported higher contribution of the CO-CO-CO process to this HW dimension than the VIS themselves, illustrated in figure 4. Lastly, the frequency of involvement in the co-deployment process does not seem to significantly affect the perceived impact on 5 HW dimensions (although we can see that the correlation coefficient with the healthy lifestyles dimension almost reached the cut-off level of α=0.05).
Conclusion
The findings from this study highlight the significant impact of inclusive public space interventions on health and well-being, particularly when co-designed, co-deployed, and co-managed with local communities. The IN-HABIT project in Nitra demonstrated that participatory urban interventions can enhance psychological well-being, foster social cohesion, and improve perceptions of spatial and environmental quality. The strongest positive effects were observed in psychological well-being, with participants reporting increased cheerfulness, engagement, and sense of purpose. However, the extent of these benefits varied depending on the characteristics and vulnerabilities of specific target groups, which underscores the importance of tailoring interventions to diverse needs.
Psychological well-being improvements were most pronounced among groups experiencing social exclusion, including migrants, refugees, and LGBTQI+ individuals, who reported increased cheerfulness, social engagement, and a stronger sense of belonging. Women and elderly participants perceived notable improvements in spatial and environmental well-being, particularly in relation to accessibility and safety, though concerns over security and inclusivity persisted. The interventions also positively influenced social well-being, with people living alone and ethnic minorities reporting increased trust in others, stronger community ties, and greater motivation to participate in local initiatives.
Social well-being emerged as a key dimension on which participatory processes—rather than the physical interventions themselves—had the greatest impact. Active involvement in co-design and co-deployment contributed to stronger community bonds, increased civic engagement, and a heightened sense of belonging. These findings suggest that participatory urban planning approaches not only improve immediate health and well-being outcomes but also contribute to long-term community resilience and empowerment.
This study reinforces the argument that inclusive urban interventions should go beyond physical transformations to prioritize meaningful community engagement. Future research should further explore how long-term involvement in co-design processes influences well-being over time and how interventions can be optimised to address the specific needs of marginalised and intersecting social groups. By embedding participatory frameworks like the CO-CO-CO approach into urban planning, cities can create more equitable, resilient, and health-promoting environments that reflect the diverse needs of all residents.
The strongest benefits were reported not merely from experiencing improved public spaces but from active participation in their design, implementation, and governance. These findings suggest that truly inclusive and impactful urban development must prioritize meaningful community participation, ensuring that interventions reflect the needs, aspirations, and lived experiences of diverse populations.
References
Agarwala, M., Atkinson, G., Fry, B., Homewood, K., Mourato, S., Rowcliffe, J. M., Wallace, G., & Milner-Gulland, E. (2014). Assessing the relationship between human well-being and ecosystem services: A review of frameworks. Conservation and Society, 12(4), 437. https://doi.org/10.4103/0972-4923.155592
Ahmimed, C. (2018). Inclusive cities: trends and new initiatives. [Presentation]. Unesco. https://www.un.org/development/desa/family/wp-content/uploads/sites/23/2018/05/UNDESA-Presentation-on-Inclusive-Cities-16-May-C.Ahmimed.pdf
Ala-Mantila, S., Heinonen, J., Junnila, S., & Saarsalmi, P. (2018). Spatial nature of urban well-being. Regional Studies, 52(7), 959-973. https://doi.org/10.1080/00343404.2017.1360485
Álvarez-Melcón, I., Sisto, R., Rodríguez, Á. D. J., & Pereira, D. (2024). Integrating the SDGs into urban regeneration: A Madrid Nuevo Norte case study using an adapted voluntary local review framework. Sustainability, 16(22), 9727. https://doi.org/10.3390/su16229727
Anderson, J., Ruggeri, K., Steemers, K., & Huppert, F. (2017). Lively social space, well-being activity, and urban design: Findings from a low-cost community-led public space intervention. Environment and Behavior, 49(6), 685-716. https://doi.org/10.1177/0013916516659108
Anderson, M., & Parker, B. (2018). Cost-benefit analysis of urban regeneration projects. Urban Studies, 55(8), 1739-1756.
Bauer, G. R. (2014). Incorporating intersectionality theory into population health research methodology: Challenges and the potential to advance health equity. Social Science & Medicine, 110, 10-17.
Belcher, B., & Palenberg, M. (2018). Outcomes and Impacts of Development Interventions: Toward Conceptual Clarity. American Journal of Evaluation, 39(4):478-495. https://doi.org/10.1177/1098214018765698
Benfer, E. A., Bhandary-Alexander, J., Cannon, Y., Makhlouf, M. D., & Pierson-Brown, T. (2021). Setting the health justice agenda: Addressing health inequity & injustice in the post-pandemic clinic. Clinical Law Review, 28(1), 45-84.
Braubach, M., Tobollik, M., Mudu, P., Hiscock, R., Chapizanis, D., Sarigiannis, D., Keuken, M., Perez, L., & Martuzzi, M. (2015). Development of a quantitative methodology to assess the impacts of urban transport interventions and related noise on well-being. International Journal of Environmental Research and Public Health, 12(6), 5792-5814. https://doi.org/10.3390/ijerph120605792
Bunnell, T. (2019). Inclusiveness in urban theory and urban-centred international development policy. Journal of Regional and City Planning, 30(2), 89-101. https://doi.org/10.5614/jpwk.2019.30.2.1
Cassarino, M., Shahab, S., & Biscaya, S. (2021). Envisioning happy places for all: A systematic review of the impact of transformations in the urban environment on the wellbeing of vulnerable groups. Sustainability, 13(14), 8086. https://doi.org/10.3390/su13148086
Collomb, J.-G. E., Alavalapati, J. R., & Fik, T. (2012). Building a multidimensional wellbeing index for rural populations in northeastern Namibia. Journal of Human Development and Capabilities, 13(2), 227-246. https://doi.org/10.1080/19452829.2011.645532
Crenshaw, K. W. (1989). Demarginalizing the intersection of race and sex: A Black feminist critique of antidiscrimination doctrine, feminist theory, and antiracist politics. University of Chicago Legal Forum, 140, 139-167.
Diener, E. (1984). Subjective well-being. In The Science of Well-Being. Social Indicators Research Series (pp. 542-75, vol. 37). Springer, Dordrecht. https://doi.org/10.1007/978-90-481-2350-6_2
Duncan, D. T., Castro, M. C., Gortmaker, S. L., Aldstadt, J., Melly, S. J., & Bennett, G. G. (2012). Racial Differences in the Built Environment—Body Mass Index Relationship? A Geospatial Analysis of Adolescents in Urban Neighborhoods. International Journal of Health Geographics 11(1):, 11. https://doi.org/10.1186/1476-072x-11-11
Evans, R. G., Barer, M. L., & Marmor, T. R. (2015). Why are some people healthy and others not? The determinants of health in populations. Aldine de Gruyter.
Fleche, S., Smith, C., & Sorsa, P. (2012). Exploring determinants of subjective wellbeing in OECD countries: Evidence from the World Value Survey. OECD Publishing. https://doi.org/10.1787/5k9ffc6p1rvb-en
Fleuret, S., & Prugneau, J. (2015). Assessing students’ wellbeing in a spatial dimension. The Geographical Journal, 181(2), 110-120. https://doi.org/10.1111/geoj.12098
Franks, D. M., Brereton D., & Moran C. J. (2011). Cumulative Social Impacts. In F. Vanclay and A. M. Esteves (eds.), New Directions in Social Impact Assessment(pp. 202-220). Edward Elgar Publishing.
Haas, B. K. (1999). Clarification and integration of similar quality of life concepts. Image-the journal of nursing scholarship, 31(3), 215-20. https://doi.org/10.1111/J.1547-5069.1999.TB00483.X
Haider, J. (2007). Inclusive design: Planning public urban spaces for children. Proceedings of the Institution of Civil Engineers - Municipal Engineer, 160(2), 83-88. https://doi.org/10.1680/muen.2007.160.2.83
Harding, A. (2014). What is the difference between an impact and an outcome? Impact is the longer term effect of an outcome. The London School of Economics. https://blogs.lse.ac.uk/impactofsocialsciences/2014/10/27/impact-vs-outcome-harding/
Harvey, D. (1973). Social justice and the city. Johns Hopkins University Press.
Helliwell, J. F., & Putnam, R.D. (2004). The social context of well-being. Philosophical transactions of the Royal Society of London. Series B, Biological Sciences,359(1449), 1435-46. https://doi.org/10.1098/rstb.2004.1522
Howell, R. T., Kern, M. L., & Lyubomirsky, S. (2007). Health benefits: Meta-analytically determining the impact of well-being on objective health outcomes. Health Psychology Review, 1, 83-136.
Itair, M., Shahrour, I., & Hijazi, I. (2023). The use of the smart technology for creating an inclusive urban public space. Smart Cities, 6(5), 2484-2498. https://doi.org/10.3390/smartcities6050112
Jennings, V., Rigolon, A., Thompson, J., Murray, A., Henderson, A., & Gragg, R. S. (2024). The dynamic relationship between social cohesion and urban green space in diverse communities: Opportunities and challenges to public health. International Journal of Environmental Research and Public Health, 21(6), 800. https://doi.org/10.3390/ijerph21060800
Jian, I. Y., Chan, E. H. W., Xu, Y., & Owusu, E. K. (2021). Inclusive public open space for all: Spatial justice with health considerations. Habitat International, 118, 102457. https://doi.org/10.1016/j.habitatint.2021.102457
Keating, D. P. (2016). Social inequality in population developmental health. Advances in Child Development and Behavior, 50, 75-104. https://doi.org/10.1016/bs.acdb.2015.12.002
Ксендзук, В. В., Власюк, Т. О., & Сергієнко, І. Г. (2023). Оцінка впливу наслідків війни на розвиток зовнішньої торгівлі товарами на урбанізованих територіях України. Економіка, управління та адміністрування, 3(105), 51-58.
Khan, N., Keck, L., Sykes, C., Rowden, C., Simister, J., Fenlon, S., Mccallum, E., Bell, M., Whiting, D., Shelton, C., Wells, G., Giles, R., Howard, J., & Peckham, S. (2024). Diversity, community engagement and co-design in research: A rapid review. BMJ Leader. https://doi.org/10.1136/leader-2024-001046
Kiefer, R. A. (2008). An integrative review of the concept of well-being. Holistic nursing practice, 22(5), 244-52. https://doi.org/10.1097/01.HNP.0000334915.16186.b2
Lam, B., Zamenopoulos, T., Kelemen, M., & Hoo Na, J. (2017). Unearth hidden assets through community co-design and co-production. The Design Journal, 20(sup1), S3601-S3610. https://doi.org/10.1080/14606925.2017.1352863
Larson, S., Stoeckl N., Jarvis D., Addison, J., Prior, S., & Esparon, M. (2019). Using measures of wellbeing for impact evaluation: Proof of concept developed with an indigenous community undertaking land management programs in northern Australia. Ambio, 48(1), 89-98. https://doi.org/10.1007/s13280-018-1058-3
Livingston, V., Jackson-Nevels, B., & Reddy, V. V. (2022). Social, cultural, and economic determinants of well-being. Encyclopedia, 2(3), 1183-1199. https://doi.org/10.3390/encyclopedia2030079
Mac Fadden, I., Cocchioni, R., & Delgado-Serrano, M. M. (2024). A co-created assessment framework to measure inclusive health and wellbeing in a vulnerable context in the south of Europe. International Journal of Environmental Research and Public Health, 21(4), 510. https://doi.org/10.3390/ijerph21040510
Marmot, M., & Allen, J. (2014). Social determinants of health and well-being in urban environments. The Lancet, 384(9939), 287-293.
Marmot, M., Stansfeld, S., & Patel, C. (2012). Health inequalities and social determinants of health. The Lancet, 380(9847), 244-252.
Maruniak, E. O., Lisovskyi, S. A., Pokliatskyi, S. A., Mozghovyi, A. A., Petrovska, A. O., & Rumiantseva, M. V. (2021). Development of the capital city through the prism of inclusiveness (A case of Kyiv). Ukrainian Geographical Journal, 1, 25-33. https://doi.org/10.15407/ugz2021.01.025
Medayese, S., Magidimisha-Chipungu, H. H., Popoola, A. A., Chipungu, L., & Adeleye, B. M. (2020). Thematic review of trends in inclusive urban development studies (2000-2020). In E. S. Osabuohien, E. A. Oduntan, O. Gershon, O. Onanuga, & O. Ola-David (Eds.), Practice, progress, and proficiency in sustainability (pp. 362-372). IGI Global. https://doi.org/10.4018/978-1-7998-4817-2.ch021
Meringolo, P., Volpi, C., & Chiodini, M . (2019). ‘Community Impact Evaluation. Telling a Stronger Story’. Community Psychology in Global Perspective, 5(1), 85-106.
Mitrašinović, M., & Mehta, V. (2021). Diversity and inclusion in public space. In M. Mitrašinović & V. Mehta (eds.). Public Space Reader (pp. 59-63). Routledge.
Можаровська, Т. (2021). Психологічне благополуччя: теоретичні підходи до визначення поняття. Psychological Prospects Journal, 37, 155-167. https://doi.org/10.29038/2227-1376-2021-37-155-167
National Institute on Aging. (2020). Health disparities in older adults. Author. https://www.nia.nih.gov/research/publication/health-disparities
Nguyen, N. T., Collins A., & Collins C. M. (2024). Trends and patterns in the application of co-production, co-creation, and co-design methods in studies of green spaces: A systematic review. Environmental Science & Policy, 152, 103642. https://doi.org/10.1016/j.envsci.2023.103642
Peters, K. (2010). ‘Being together in urban parks: Connecting public space, leisure, and diversity. Leisure Sciences, 32(5), 418-33. https://doi.org/10.1080/01490400.2010.510987
Prilleltensky, I., Dietz, S., Prilleltensky, O., Myers, N. D., Rubenstein, C. L., Jin, Y., & McMahon, A.. (2015). Assessing Multidimensional well-being: Development and Validation of the I Coppe Scale. Journal of Community Psychology, 43(2), 199-226. https://doi.org/10.1002/jcop.21674
Rishbeth, C. (2001). ‘Ethnic minority groups and the design of public open space: An inclusive landscape? Landscape Research, 26(4), 351-366. https://doi.org/10.1080/01426390120090148
Robert, G., Locock, L., Williams, O., Cornwell, J., Donetto, S., & Joanna Goodrich. (2022). Co-Producing and Co-Designing. (1st ed). Cambridge University Press.
Romanelli, M. (2022). Towards Smart Inclusive Cities. PuntOrg International Journal, 7(2), 216-234. https://doi.org/10.19245/25.05.pij.7.2.6
Salsabila, S., & Navitas, P. (2024). Built environment design features, mental health, and well-being for inclusive urban design: An extensive literature review. IOP Conference Series: Earth and Environmental Science, 1394(1), 012020.
Sarriera, J. C., & Bedin, L. M. (2017). A Multidimensional Approach to Well-Being. InJ. C. Sarriera & L. M. Bedin (eds.), Psychosocial Well-being of Children and Adolescents in Latin America. Vol. 16, Children’s Well-Being: Indicators and Research (pp. 3-26). Springer International Publishing.
Schonhardt, S., Sullivan, S., Shisler Marshall, R. (2023). ‘A Focused Review of Multidimensional Well-Being Assessments’. Journal of Wellness, 4(2). https://doi.org/10.55504/2578-9333.1140
Sfeatcu, R., Cernuşcă-Miţariu, M., Ionescu, C., Roman, M., Cernuşcă-Miţariu, S., Coldea, L., Boța, G., & Burcea, C. (2014). The Concept of Wellbeing in Relation to Health and Quality of Life. European Journal of Science and Theology, 10(4), 123-128.
Sirgy, M. J. (2021). ‘Effects of Demographic Factors on Wellbeing’. In The Psychology of Quality of Life. Social Indicators Research Series (pp. 129-54, vol. 83). Springer International Publishing.
Soja, E.W. (2010). Seeking Spatial Justice. University of Minnesota Press.
Thomas, G., Lynch, M., & Spencer, L. H. (2021). A Systematic Review to Examine the Evidence in Developing Social Prescribing Interventions That Apply a Co-Productive, Co-Designed Approach to Improve Well-Being Outcomes in a Community Setting. International Journal of Environmental Research and Public Health, 18(8), 3896. https://doi.org/10.3390/ijerph18083896
Wolff, E., & Zacharias, A. (2003). Well-being in America: The Levy Institute measure of economic well-being. Indicators, 2(4), 44-73. https://doi.org/10.1080/15357449.2003.11069178
Notes
*
Artículo de investigación / Research
article
Origin of this Research
This research was funded under
the IN‐HABIT (INclusive Health And wellBeing In small and medium size ciTies) Project
as part of the Horizon 2020 Program (Grant Agreement No. 869227). The content
of this document does not reflect the official opinion of the European Union.
Responsibility for the information and views expressed herein lies entirely
with the authors.
Author notes
a Autora de correspondencia / Correspondence author. E-mail: xhodnieva@uniag.sk
Additional information
Cómo citar
/ How to cite: Hodnieva, Y., Melichová, K., Bellérová, S., & Popovicsová,
J. K. (2025). Stakeholder Evaluation of Health and Wellbeing Outcomes of
Inclusive Public Space Interventions Delivered by the IN-HABIT Project. Cuadernos
de Vivienda y Urbanismo, 18. https://doi.org/10.11144/Javeriana.cvu18.sehw
