








APA
ISO 690-2
Harvard
Haga clic en un formato de citación
A Competency-based Approach to Promoting Effective Hand Hygiene in Long-term Care Facilities*
Un enfoque basado en la competencia para promover la higiene de las manos eficaz en los centros de atención a largo plazo
Uma abordagem baseada na competência para promover a higiene das mãos eficaz em centros de atenção em longo prazo
Daniel A. Nnate
A Competency-based Approach to Promoting Effective Hand Hygiene in Long-term Care Facilities*
Investigación en Enfermería: Imagen y Desarrollo, vol. 24, 2022
Pontificia Universidad Javeriana
Daniel A. Nnate, BSc (Hons), MPH, MSN, RN a DNNATE200@caledonian.ac.uk
School of Health and Life Sciences, United Kingdom
Department of Nursing and Community Health, School of Health and Life Sciences, Glasgow Caledonian University, United Kingdom
Countess of Chester Hospital NHS Foundation Trust, Liverpool Road, Chester, CH2 1UL, United Kingdom
Received: 22 july 2021
Accepted: 21 january 2022
Published: 30 january 2022
Abstract:
Introduction: Long-term care facilities comprise a large proportion of healthcare service users due to the increasing ageing population. Healthcare-associated infections constitute a major burden in long-term care facilities and are associated with significant infectious disease outbreaks and mortality. The non-adherence to effective hand hygiene practice due to missed opportunities for staff to explore its role in infection prevention and control within these settings has been emphasised by the Covid-19 pandemic.
Methods: This article is designed to assist the continuing professional development needs of nursing and associate professionals in long-term care facilities. It explores the factors contributing to the poor attitude of staff members towards non-compliance with infection prevention and control measures in long-term care facilities.
Results: Recommendations for improving infection prevention and control measures were further made based on the Infection Prevention Society competency framework which serves as a tool for individuals to improve their performance continually and become efficient practitioners.
Conclusion: After reading this article, healthcare practitioners should be able to (i) identify various means of promoting adequate hand hygiene in long-term care facilities; (ii) understand that every activity taken to prevent the spread of healthcare-associated infections begins and ends with effective hand hygiene; (iii) recognise steps to prevent cross-infection through improved compliance with the five moments of hand hygiene in long-term care facilities; (iv) develop a satisfactory attitude towards hand hygiene compliance in the workplace, and (v) appraise own competence, and promote staff compliance through feedback.
Keywords:hand hygiene, healthcare-associated infection, infection prevention, long-term care, preventive health services.
Resumen:
Introducción: Los centros de cuidados de larga duración representan una gran proporción de usuarios de servicios sanitarios debido al creciente envejecimiento de la población. Las infecciones asociadas a la asistencia sanitaria constituyen una carga importante en los centros de asistencia de larga duración y están asociadas a importantes brotes de enfermedades infecciosas y a la mortalidad. La falta de adherencia a la práctica efectiva de la higiene de manos debido a la pérdida de oportunidades para que el personal explore su papel en la prevención y el control de las infecciones dentro de estos entornos ha sido enfatizada por la pandemia de COVID-19.
Métodos: Este artículo está diseñado para ayudar a las necesidades de desarrollo profesional continuo de los profesionales de enfermería y asociados en los centros de cuidados de larga duración. Explora los factores que contribuyen a la mala actitud de los miembros del personal hacia el incumplimiento de las medidas de prevención y control de infecciones en los centros de cuidados de larga duración.
Resultados: Se formularon además recomendaciones para mejorar las medidas de prevención y control de las infecciones basadas en el marco de competencias de la Sociedad de Prevención de Infecciones, que sirve de herramienta para que los individuos mejoren continuamente su rendimiento y se conviertan en profesionales eficientes.
Conclusión: Después de leer este artículo, los profesionales sanitarios deberían ser capaces de (i) identificar diversos medios para promover una adecuada higiene de las manos en los centros de cuidados de larga duración; (ii) comprender que toda actividad realizada para prevenir la propagación de las infecciones asociadas a la asistencia sanitaria comienza y termina con una higiene de las manos eficaz; (iii) reconocer los pasos para prevenir la infección cruzada mediante un mejor cumplimiento de los cinco momentos de la higiene de las manos en los centros de cuidados de larga duración; (iv) desarrollar una actitud satisfactoria hacia el cumplimiento de la higiene de las manos en el lugar de trabajo, y (v) evaluar la propia competencia, y promover el cumplimiento del personal mediante la retroalimentación.
Palabras clave: higiene de manos, infección asociada a la atención sanitaria, prevención de infecciones, cuidados de larga duración, servicios sanitarios preventivos.
Resumo:
Introdução: Os centros de cuidados de longa duração representam uma grande proporção de usuários de serviços sanitários devido ao crescente envelhecimento da população. As infeções associadas à assistência sanitária constituem um fardo significativo em centros de assistência de longa duração e estão associadas a importantes surtos de doenças infeciosas e à mortalidade. A falta de adesão à prática efetiva da higiene de mãos devido à perda de oportunidades para o pessoal explorar o seu papel na prevenção e controle das infeções dentro desses ambientes já foi enfatizada pela pandemia de COVID-19.
Métodos: Este artigo foi desenhado para ajudar às necessidades de desenvolvimento profissional continuo dos profissionais de enfermagem e associados nos centros de cuidados de longa permanencia. Explora os fatores que contribuem para as más atitudes dos funcionários para o não cumprimento das medidas de prevenção e controle de infeções nos centros de cuidados de longa duração.
Resultados: Foram formuladas também recomendações para melhorar as medidas de prevenção e controle das infeções baseadas no quadro de competências da Sociedade de Prevenção de Infeções, que serve de ferramenta para que os indivíduos melhorem continuamente seu desempenho e se tornem profissionais eficientes.
Conclusão: Após a leitura deste artigo, os profissionais sanitários devem ser capazes de (i) identificar diversos meios para promover uma adequada higiene das mãos nos centros de cuidados de longa duração; (ii) entender que toda atividade realizada para prevenir a propagação das infeções associadas à assistência sanitária começa e termina com uma higiene eficaz das mãos; (iii) reconhecer os passos para prevenir a infeção cruzada por meio de uma melhor adesão aos cinco momentos da higiene das mãos em centros de cuidados de longa duração; (iv) desenvolver uma atitude satisfatória em relação à adesão da higiene das mãos no local de trabalho, e (v) avaliar a própria competência, e promover a adesão da equipe mediante a retroalimentação.
Palavras-chave: higiene de mãos, infeção associada à atenção sanitária, prevenção de infeções, cuidados de longa duração, serviços sanitários preventivos.
Introduction
Long-term care facilities (LTCFs) comprise a large proportion of the healthcare systems globally due to the increasing ageing population. These settings primarily serve older patients, who are associated with higher levels of multi-morbidity (1). Long-term care facilities may likely constitute a breeding ground for Healthcare-associated infections (HAIs) where strict adherence to infection prevention and control (IPC) measures are not followed. Frequently isolated microorganisms in LTCFs such as Escherichia coli, Streptococcus pneumoniae, Staphylococcus aureus, Candida spp. and Pseudomonas aeruginosa can be readily transmitted from one individual to another through inadequate hand hygiene practice (2). While these opportunistic organisms make up the normal microbiome of the gut and skin, they are likely to cause severe infection in individuals with a weak immune system or when they are introduced into susceptible organs (3).
Although common issues on infection prevention and control in LTCF ranges from funding, staff shortage, high staff turnover, and poorly structured guidelines for IPC (4-5), challenges related to poor operational structures, inability to implement fundamental IPC guidelines, low compliance rate and adopting a structured means of assessing staff competencies was further emphasised by Nguyen et al. (4). On the operational level, nurses, care support staff, and cleaners play a major role in implementing efficient and safe IPC measures in LTCFs. For instance, in the United Kingdom and United States, nursing homes, residential homes, hospices, and home care services are primarily run by nurses and nurse assistants (6-7). In this care environment, it becomes important that staff members adhere to recommended standard precautions for IPC (8-9). These standards for IPC aim to promote patient safety, which can only be achieved when healthcare professionals adhere to the guidelines, which greatly emphasise effective hand hygiene.
Hand hygiene and personal protective equipment (PPE)
Hand hygiene is the primary measure that has been proven to be effective in preventing HAIs, and as such, there is great emphasis on hand hygiene with soap and water or hand gel as a means for IPC (10). Effective hand hygiene is recommended before and after each contact with a patient, after touching the patient’s surrounding area, before performing an aseptic procedure, and after exposure to bodily fluids (11). Together, these are known as the five moments for hand hygiene. (See: https://bit.ly/Your_5_Moments). It is important to note that hand decontamination with soap and water is the standard recommended method when hands are visibly dirty or soiled. In case of Clostridium difficile infection, vomiting or a diarrhoeal illness, Loveday et al. (12) emphasised that hand decontamination with soap and water should be performed before and after patient contact irrespective of whether gloves have been worn. This is because alcohol-based handrub is ineffective against C. difficile. All other clinical situations, for example before and after patient contact, should see hands sanitised with an alcohol-based handrub (10,13). Although standard hand hygiene practice is often sufficient, it is worth considering other activities or moments where hand hygiene may be appropriate for HCWs. For instance, fomites such as the patient’s clothes, bedrails, mobile aids, utensils, and table surface are also likely to harbour microorganisms.
Additional opportunities for hand hygiene come into play where a handwashing facility is in the patient’s room. Considering the barrier that exists between the patient's room and the surrounding environment, there are also potentials for bacteria to reside on light switches or door handles, and hand hygiene may be required after its use. While hand hygiene after these activities could further reduce infection rates, it may not be realistic in a busy healthcare environment. The strict implementation of the 5 components of the WHO (14) multimodal strategy to improve hand hygiene has been emphasised to mitigate these lapses. Components of the multimodal strategy for hand hygiene includes access to a safe hand washing facility at the point of care, continuous staff training and feedback, reminders in the workplace and an organisation that promotes patient safety.
The Global COVID-19 pandemic has necessitated a more extensive use of personal protective equipment (PPE) for HCWs, including those working in LTCFs. Similar to other lethal respiratory tract infections such as influenza (from strains A and B), pneumonia, bronchitis, bronchiolitis and severe acute respiratory syndrome (SARS), droplets can survive on surfaces and are transmitted when a contaminated hand touches the eyes, nose, or mouth (15). Hand hygiene must be performed and extended to exposed forearms after removing PPE such as aprons, gloves, masks and after administering supplemental oxygen. Although the evidence base for promoting good respiratory hygiene as a major infection control measure is well established, it is also important to note that effective hand hygiene practice complements respiratory hygiene (see: https://bit.ly/catch-bin-kill). Much emphasis has been placed on hand hygiene as a means of mitigating HAIs because every IPC measure taken to prevent the spread of infection begins and ends with effective hand hygiene.
Activity
Reflect on ways you could promote effective infection prevention and control practices at your workplace. This includes necessary measures to be taken in minimising cross-infection between healthcare service users and compliance with hand hygiene requirements.
Factors influencing compliance with hand hygiene in LTCF
An enquiry into factors contributing to the non-compliance of hand hygiene reveals that human behaviour was attributed to the observed lapses. Good hand hygiene should be considered a habit. This cognitive process has been extensively studied using the theory of planned behaviour (conscious behaviours) to explore human factors such as the perceived intention which is influenced by attitude, subjective norms, and level of control over a situation at any given time (16). Therefore, knowledge of the consequence of not engaging in a behaviour is the major driving factor for engaging in such behaviour. In addition, the social norms behind these actions are often embedded in the organisational goals which suggest good role modelling by staff members.
As humans, our beliefs tend to shape how we think, which further determine our habits and everyday activities. Less conscious human behaviours often lead to promoting or less prioritisation of hand hygiene in the workplace (17-18). The feeling of disgust, responding to audits and the belief of protecting oneself and other HCW and service users is a driving factor for carrying out effective hand hygiene (16,18). In contrast, perceived lack of control over other factors such as time constraints, workload, frequent interruption, skin irritation and glove preference are barriers to effective hand hygiene (16,19-20). A common knowledge-based error often encountered during hand hygiene is non-compliance with all the steps involved in hand decontamination. This is a matter of concern as there is a strong belief among HCWs that hand hygiene has been performed, despite not being carried out effectively.
Gluyas (17) highlighted that errors resulting from deliberate and non-deliberate violations while undertaking hand hygiene may occur. Some violations are also accompanied by an assessment of the low risk involved in not performing hand hygiene. For instance, research shows that HCWs perceive non-compliance with two of the five moments for hand hygiene –before touching a patient, and after touching the surrounding area of a patient– as less risky than some of the other moments (17,21). Similarly, McLaughlin et al. (22) found that healthcare workers perceive the risk of cross-infection to be low after touching surfaces. More recent evidence by Stephens et al. (23) has revealed that pathogenic microorganisms are present in high levels on surfaces with human occupancy.
Activity
Consider the steps taken to effectively perform hands hygiene. Although these steps are supposed to be performed with minimum conscious thought, reflect on how often each step is completed. (See: https://bit.ly/hand-hygiene-information).
Cognitive performance of hand hygiene is often affected by much familiarity with the task and coping with adjustment in work situations, and there is a high tendency of staff to work around evidence-based guidelines. Although strategic placing of infographics on the procedure for performing effective hand hygiene is likely to minimise errors observed during routine hand hygiene, prior reflection on such activity should be encouraged to enhance the cognitive process. However, according to McLaughlin et al. (22), it is almost certain that in life-saving situations, such as preventing falls and assisting a choking patient, where compliance with hand hygiene may be challenging, HCWs may not miss the opportunity to carry out hand hygiene if they perceive any risk to themselves. Moreover, while some of these slips and lapses are in response to exceptional circumstances which are beyond their control, others may be deliberate due to the lack of knowledge, poor role modelling or little organisational support (17,24). Another form of non-compliance is the excessive use of gloves or the belief in using gloves as a substitute for hand hygiene. In this regard, appropriate hand hygiene after the use of gloves in healthcare settings has been emphasised by several authors (25-26). The aim is to reduce the colonisation of microorganisms on the palm and wrist which often result from inappropriate donning and doffing of hand gloves.
Several environmental factors have been linked to low compliance with hand hygiene in healthcare. Time constraints for staff are frequently cited in the literature as one of the biggest factors that prevent compliance with hand hygiene (18-19,27). As well as time, Gluyas and Morrison (27) identified inadequate knowledge on IPC and pressure due to increased workload as negative factors. It was also recognised that the structure and layout of some facilities may not promote effective infection prevention and hand hygiene. For example, poor siting of sanitising gel dispensers, sluice and washbasins may likely not suit the work plan of HCWs. White et al. (16) identified the availability of facilities themselves as one of the most frequently reported factors which negatively influenced compliance.
Improving compliance with hand hygiene using the competency framework for IPC practitioners
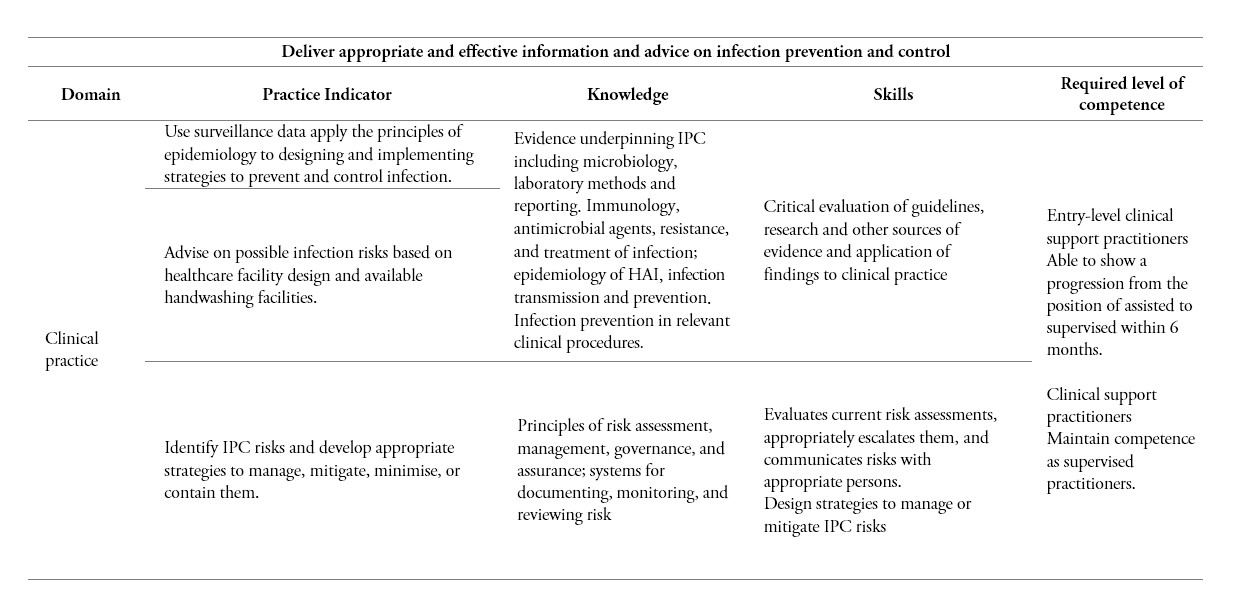
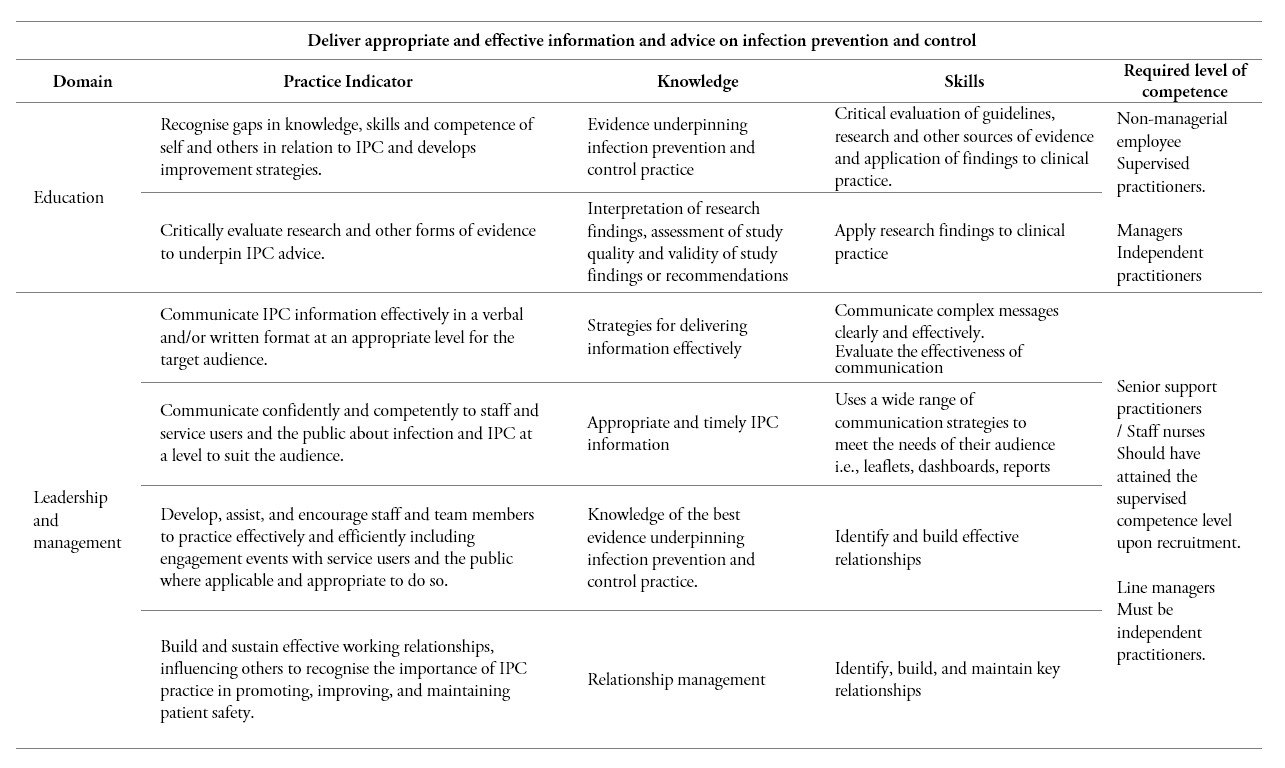
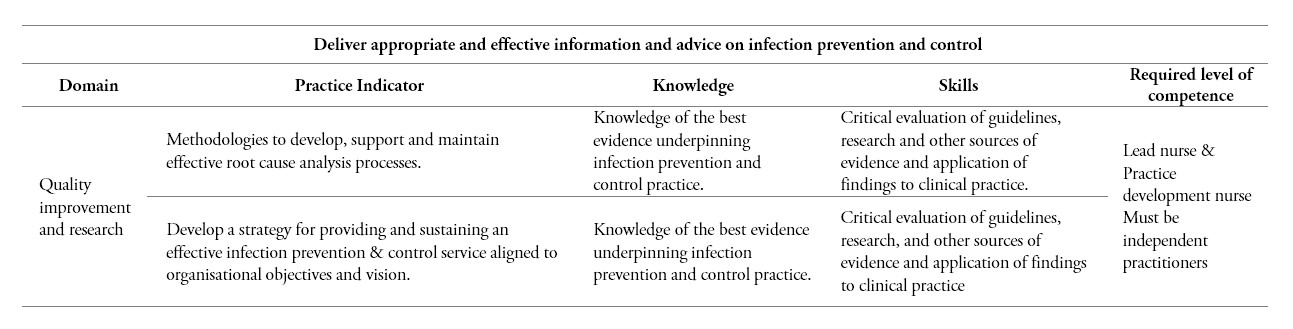
Competencies are demonstrated ability to apply knowledge, skills, and attitudes for personal development to achieve observable results. These motives and personal traits often exhibited by individuals help them evaluate how they perform certain tasks. In 2011, the Infection Prevention Society (IPS) developed a framework to enable IPC practitioners to enhance their knowledge and skills to help increase patient safety and quality of care (8). This framework which comprises four core competencies and domains can aid in assessing education programmes, staff appraisal and review of organisational structures to determine areas for improvement and further training requirements. The competency framework and domains comprise (i) clinical practice; (ii) quality improvement & research; (iii) education; and (v) leadership and management. Table 1 provides guidance on the knowledge and skill that staff members responsible for the development and implementation of IPC measures in LTCFs should have, in order to carry out their responsibilities. Particular emphasis was paid to the IPS core competencies because it gives a summary of the skill base required for effective practice in specific job roles. This also coincides with the step-wise approach to implementing the WHO (14) multimodal hand hygiene improvement strategy which is (i) facility preparedness; (ii) baseline evaluation; (iii) implementation; (iv) follow-up evaluation; and (v) review and planning. Furthermore, recommendations for improving hand hygiene compliance in the workplace were made based on the multimodal improvement strategy.
Support for improving compliance with IPC in LTCFs
Insufficient time, poor knowledge, and pressure due to increased workload and organisational barriers have been attributed to the noncompliance with effective hand hygiene. In the light of the contributing factors to non-compliance with hand hygiene discussed in the previous section, various studies recommended that a habit of effective hand hygiene can be formed with practice (18,28-29). It was further emphasised that the development of habitual hand hygiene practices as unconscious automated behaviour could lead to better compliance with IPC measures (18). According to Lally et al. (30), it can take between 18 to 254 days for a behaviour to transform into a habit. While this period is highly subjective to the individual, Lee et al. (31) also observed that repetitive theoretical and practice sessions lead to a significant improvement of the HCW’s competencies in IPC in their workplace. Gluyas (17) also emphasised the need for senior healthcare staff to act as role models in promoting hand hygiene in their workplaces. It was further suggested that a lack of role modelling could contribute to low levels of compliance with all 5 moments of hand hygiene by staff members (17). Hence, there is the need to develop a competency-based framework for training healthcare support workers in IPC.
While evidence underpinning IPC such as epidemiology of HAI, infection transmission and prevention procedures are basic requirements for an entry-level practitioner which can be developed further through practice and education. Lee et al. (31) identified that education, monitoring, and feedback were components of an IPC training programme that resulted in significant behavioural change within healthcare staff in LTCFs. Koo et al. (32) also highlighted how training can influence compliance, with self-reported compliance with hand hygiene independently associated with the receipt of training and participation in a previous hand hygiene campaign. It is however certain that progressing from one competency level to another provides IPC practitioners with the ability to display evidence of IPC competencies expected in a previous role, as well as their willingness to work towards specialist advanced competencies.
Giving timely feedback as a means of motivating and empowering staff to continue with optimal hand hygiene practice have been recommended in various literature (33-34). While this approach is likely to encourage good practice, Burnett (35) suggested that feedback provided to staff should focus on hand hygiene compliance rather than non-compliance, as this is more likely to impede the personal development of defaulting staff. Lee et al. (31) have also suggested that frequent training, continuous audits, and timely feedback bring about behavioural change amongst HCWs working in LTCFs. Furthermore, considering the role of audits in IPC, Erasmus et al. (21) and Srigley et al. (34) advised that a positive response resulting from an awareness of being assessed is likely to bring about a behaviour change. Therefore, positive feedback on IPC compliance also provides support for behaviour change as junior staff members are most likely to change practice with motivation from their senior colleagues.
Storr et al. (33) recommended a series of best practice elements for effective infection prevention and control programmes in line with WHO recommendations. These comprise implementing efficient IPC programmes, continuous training, monitoring and feedback, and adequate institutional support. In this paper, the author recommended an integration of the IPC competencies as an approach to implementing the WHO multimodal strategy. Working through the assisted, supervised, and independent competency levels further enable practitioners to meet evidence-based recommendations proffered in recent literature on hand hygiene compliance (33,36). The competencies also promote self-reported compliance with hand hygiene which is independently associated with receipt of training and participation in previous hand hygiene campaigns.
In the recently published report by the WHO (36) on promoting quality health care, it was revealed that inadequate access to handwashing facilities and poor hand hygiene habits in health care settings suggests that good IPC practices may be difficult to implement. Surprisingly, poor positioning of handwashing facilities and the inability to access alcohol-based handrub at the point of care were identified as factors that impede recommended IPC practices (36). These findings reflect those of Salcedo-Cifuentes et al. (37) who also reported that hand hygiene compliance goes beyond good habits but also the availability of handwashing sinks or alcohol-based disinfectants at the point of care, and proper management. In addition to the availability of hand hygiene facilities, its visibility is also an important factor that is likely to increased handwashing practices. Thus, the positioning of hand hygiene stations should be strategically considered when planning and redesigning healthcare facilities.
In using the IPC framework, HCWs are able to adopt components of the multimodal strategy for hand hygiene. Achieving the required level of competence that corresponds with the education and clinical practice domains implies that access to a safe hand washing facility at the point of care and continuous staff training is guaranteed. Efficient leadership and management within the healthcare team further encourages constructive feedback in the workplace. In this regard, where the knowledge and skills corresponding to quality improvement and research domain have been met, it may then be considered that the organisation adheres to promoting patient safety in its day-to-day activities.
Conclusions and recommendations for effective practice
This paper has argued that nurses and nursing assistants play a major role in delivering safe and effective care in LTCFs. While these facilities make up a valuable proportion of the healthcare systems globally, it becomes important to establish at least the minimum IPC requirements, which represent a strong knowledge base for developing effective competencies. The author’s practice recommendations are based on the WHO step-wise approach to implementing the multimodal hand hygiene improvement strategy. While senior HCWs often serve as role models for other junior staff through education and mentoring at the point of care, they should also be able to influence behaviour towards efficient hand hygiene practices. Furthermore, it is important that senior practitioners recognise any skill gaps within the IPC team and contribute towards the personal development of team members. Therefore, assisting practitioners who may be new to infection prevention and control to develop their knowledge and skills should be the first call of action with regards to building an institutional safety climate. A practitioner who may require observation and direction to carry out a specific task or unfamiliar role must be supported with constructive feedback. As a step-wise approach to maintaining effective IPC strategy, providing appropriate infrastructures, giving timely feedback on hand hygiene compliance, and providing an enabling environment are critical elements that should form key performance indicators in LTCFs.
Funding
No funding was received for this study.
Conflict of interest statement
The authors declare no conflict of interest. The opinions expressed are the authors’ own and not those of their employers, or any other organisation.
References
1. Marengoni A, Angleman S, Melis R, Mangialasche F, Karp A, Garmen A, et al. Aging with multimorbidity: A systematic review of the literature. Ageing Res Rev. 2011;10(4):430-9. doi: 10.1016/j.arr.2011.03.003
2. Nucleo E, Caltagirone M, Marchetti VM, D’Angelo R, Fogato E, Confalonieri M, et al. Colonization of long-term care facility residents in three Italian Provinces by multidrug-resistant bacteria. Antimicrob Resist Infect Control. 2018;7(1):33. doi: 10.1186/s13756-018-0326-0
3. Price LB, Hungate BA, Koch BJ, Davis GS, Liu CM. Colonizing opportunistic pathogens (COPs): The beasts in all of us. PLoS Pathog. 2017;13(8):e1006369. doi: 10.1371/journal.ppat.1006369.
4. Nguyen LKN, Megiddo I, Howick S. Challenges of infection prevention and control in Scottish long-term care facilities. Infect Control Hosp Epidemiol. 2020;41(8):943-5. doi: 10.1017/ice.2020.113
5. Hossain MM, Mazumder H, Tasnim S, Nuzhath T, Sultana A. Geriatric Health in Bangladesh during COVID-19: Challenges and Recommendations. J Gerontol Soc Work. 2020;63(6-7):724-7. doi: 10.1080/01634372.2020.1772932.
6. Kadri A, Rapaport P, Livingston G, Cooper C, Robertson S, Higgs P. Care workers, the unacknowledged persons in person-centred care: A secondary qualitative analysis of UK care home staff interviews. PLoS One. 2018;13(7):e0200031. doi: 10.1371/journal.pone.0200031
7. Centers for Disease Control and Prevention. Nursing Homes and Assisted Living (Long-term Care Facilities [LTCFs]) [Internet]. National Center for Emerging and Zoonotic Infectious Diseases (NCEZID). 2020. Available from: https://www.cdc.gov/longtermcare/index.html (accessed 2021 Dec 31).
8. Burnett E. Outcome competences for practitioners in infection prevention and control: Infection prevention society and competency steering group. J Infect Prev. 2011;12(2):67-90. doi: 10.1177/1757177410395797
9. Nursing and Midwifery Council. The Code: Standards of conduct, performance and ethics for nurses and midwives [Internet]. Nursing and Midwifery Council. 2018. Available from: https://www.nmc.org.uk/globalassets/sitedocuments/nmc-publications/nmc-code.pdf (accessed 2021 Dec 31).
10. World Health Organisation. WHO guidelines on hand hygiene in health care: first global patient safety challenge: clean care is safer care [Internet]. Geneva, Switzerland; 2009. Available from: https://www.ncbi.nlm.nih.gov/books/NBK144013 (accessed 2021 Dec 31).
11. World Health Organisation. Hand hygiene: Why, how & when? Save lives: Clean your hands [Internet]. Geneva, Switzerland; 2009. Available from: https://www.who.int/gpsc/5may/Hand_Hygiene_Why_How_and_When_Brochure.pdf (accessed 2021 Dec 31).
12. Loveday HP, Wilson JA, Pratt RJ, Golsorkhi M, Tingle A, Bak A, et al. Epic3: National evidence-based guidelines for preventing healthcare-associated infections in nhs hospitals in england. J Hosp Infect. 2014;86(S1). doi: 10.1016/S0195-6701(13)60012-2
13. World Health Organisation. Frequently asked questions. Save lives: Clean your hands [Internet]. Geneva, Switzerland; 2010. Available from: https://www.who.int/gpsc/5may/PS_faq5mai_2010_47_en.pdf?ua=1 (accessed 2021 Dec 31).
14. World Health Organisation. Guide to the implementation. A guide to the implementation of the WHO multimodal hand hygiene improvement strategy [Internet]. 2009. Available from: http://www.who.int/gpsc/5may/Guide_to_Implementation.pdf (accessed 2021 Dec 31).
15. Department of Health and Social Care. Guidance on COVID-19: infection prevention and control [Internet]. 2020. Available from: https://www.gov.uk/government/publications/wuhan-novel-coronavirus-infection-prevention-and-control (accessed 2021 Dec 31).
16. White KM, Jimmieson NL, Obst PL, Graves N, Barnett A, Cockshaw W, et al. Using a theory of planned behaviour framework to explore hand hygiene beliefs at the “5 critical moments” among Australian hospital-based nurses. BMC Health Serv Res. 2015;15(1):1-9. doi: 10.1186/s12913-015-0718-2
17. Gluyas H. Understanding non-compliance with hand hygiene practices. Nurs Stand. 2015;29(35):40-6. doi: 10.7748/ns.29.35.40.e9929
18. Kupfer TR, Wyles KJ, Watson F, La Ragione RM, Chambers MA, Macdonald AS. Determinants of hand hygiene behaviour based on the Theory of Interpersonal Behaviour. J Infect Prev. 2019;20(5):232-7. doi: 10.1177/1757177419846286
19. Smith JD, Corace KM, MacDonald TK, Fabrigar LR, Saedi A, Chaplin A, et al. Application of the Theoretical Domains Framework to identify factors that influence hand hygiene compliance in long-term care. J Hosp Infect. 2019;101(4):393-8. doi: 10.1016/j.jhin.2018.12.014
20. Chatfield SL, DeBois K, Nolan R, Crawford H, Hallam JS. Hand hygiene among healthcare workers: A qualitative meta summary using the GRADE-CERQual process. J Infect Prev. 2017;18(3):104-20. doi: 10.1177/1757177416680443
21. Erasmus V, Daha TJ, Brug H, Richardus JH, Behrendt MD, Vos MC, et al. Systematic Review of Studies on Compliance with Hand Hygiene Guidelines in Hospital Care. Infect Control Hosp Epidemiol. 2010;31(3):283-94. doi: 10.1086/650451
22. McLaughlin AC, Walsh F, Bryant M. Effects of knowledge and internal locus of control in groups of health care workers judging likelihood of pathogen transfer. Hum Factors. 2013;55(4):803-14. doi: 10.1177/0018720813476546
23. Stephens B, Azimi P, Thoemmes MS, Heidarinejad M, Allen JG, Gilbert JA. Microbial Exchange via Fomites and Implications for Human Health. Curr Pollut Reports. 2019;5(4):198-213. doi: 10.1007/s40726-019-00123-6
24. Seo HJ, Sohng KY, Chang SO, Chaung SK, Won JS, Choi MJ. Interventions to improve hand hygiene compliance in emergency departments: a systematic review. J Hosp Infect. 2019;102(4):394-406. doi: 10.1016/j.jhin.2019.03.013
25. Picheansanthian W, Chotibang J. Glove utilization in the prevention of cross transmission: a systematic review. JBI database Syst Rev Implement reports. 2015;13(4):188-230. doi: 10.11124/jbisrir-2015-1817
26. Ford C, Park LJ. How to apply and remove medical gloves. Br J Nurs. 2019;28(1):26-8. doi: 10.12968/bjon.2019.28.1.26
27. Gluyas H, Morrison P. Patient Safety: An Essential Guide. London, United Kingdom: Palgrave Macmillan; 2013.
28. Smiddy MP, O’Connell R, Creedon SA. Systematic qualitative literature review of health care workers’ compliance with hand hygiene guidelines. Am J Infect Control. 2015;43(3):269-74. doi: 10.1016/j.ajic.2014.11.007
29. Dyson J, Lawton R, Jackson C, Cheater F. Does the use of a theoretical approach tell us more about hand hygiene behaviour? the barriers and levers to hand hygiene. J Infect Prev. 2011;12(1):17-24. doi: 10.1177/1757177410384300
30. Lally P, Van Jaarsveld CHM, Potts HWW, Wardle J. How are habits formed: Modelling habit formation in the real world. Eur J Soc Psychol. 2010;40(6):998-1009. doi: 10.1002/ejsp.674
31. Lee MH, Lee GA, Lee SH, Park YH. Effectiveness and core components of infection prevention and control programmes in long-term care facilities: a systematic review. J Hosp Infect. 2019;102(4):377-93. doi: 10.1016/j.jhin.2019.02.008
32. Koo E, McNamara S, Lansing B, Olmsted RN, Rye RA, Fitzgerald T, et al. Making infection prevention education interactive can enhance knowledge and improve outcomes: Results from the Targeted Infection Prevention (TIP) Study. Am J Infect Control. 2016;44(11):1241-6. doi: 10.1016/j.ajic.2016.03.016
33. Storr J, Twyman A, Zingg W, Damani N, Kilpatrick C, Reilly J, et al. Core components for effective infection prevention and control programmes: New WHO evidence-based recommendations. Antimicrob Resist Infect Control. 2017;6(1):1-18. doi: 10.1186/s13756-016-0149-9
34. Srigley Dr JA, Furness C, Baker GR, Gardam M. Quantification of the hawthorne effect in hand hygiene compliance monitoring using an electronic monitoring system: A retrospective cohort study. BMJ Qual Saf. 2014;23(12):974-80. doi: 10.1136/bmjqs-2014-003080
35. Burnett E. Effective infection prevention and control: the nurse’s role. Nurs Stand. 2018;33(4):68-72. doi: 10.7748/ns.2018.e11171
36. World Health Organisation. Hand hygiene for all initiative: Improving access and behaviour in health care facilities [Internet]. Geneva, Switzerland; 2020. Available from: https://apps.who.int/iris/bitstream/handle/10665/336023/9789240011618-eng.pdf?sequence=1&isAllowed=y (accessed 2021 Dec 31).
37. Salcedo-Cifuentes M, Ordóñez-Hernández CA, Calvo-Soto AP. Compliance with a hand hygiene strategy in healthcare settings. Investig en Enfermería Imagen y Desarro. 2020;22. doi: 10.11144/Javeriana.ie22.cehm.
Notes
*
Research article.
Author notes
Corresponding author. E-mail: dnnate200@caledonian.ac.uk
Additional information
How to cite this article: Nnate DA. A competency-based approach to promoting effective hand hygiene in long-term care facilities. Investig Enferm Imagen Desarr. 2022;24. https://doi.org/10.11144/Javeriana.ie24.cbap
