Introduction
Social scientists in the healthcare industry have recognized, for nearly forty years, that healthcare systems and the conditions in which people are born, grow, live, work, and age (collectively known as “social determinants”) profoundly and definitively influence the health of individuals and of populations in general (1). Several publications have illustrated the role of social determinants in producing healthcare inequities. For instance, in 2003, the United States Institute of Medicine produced the first comprehensive report showing that racial and ethnic minorities have less access to quality healthcare (2). In 2008, the World Health Organization announced a new global agenda for equity in healthcare, based on which it clearly stated and substantiated that the social determinants of healthcare, shaped by the distribution of power and material resources, work to produce many avoidable inequities in healthcare (1). In 2010, the US Centers for Disease Control and Prevention produced a white paper that called for new approaches, beyond individual interventions, to reduce healthcare disparities in HIV, viral hepatitis, sexually transmitted diseases, and tuberculosis (3). Analyzes within and between countries show that social determinants, such as gender, occupation, income, and ethnicity, can radically influence health outcomes to create hierarchies of health and disease (1,2).
The methodological implications of using an intersectional approach are extensive, and entire texts have been devoted mainly to this topic: traditional biomedical methodologies aimed at studying disaggregation methods or variables, such as multivariate predictive models. These methods seek to explain the relationship between discrete independent variables, but fail to indicate why these relationships occur, and they do not report on the social and context-dependent constructions or power structures within those relationships. Others have suggested that intersectional approaches have an affinity with traditional qualitative methodological approaches, such as ethnography or case study accounts (4).
In her paper, Kelly dismissed the strictly dichotomous intersectional view of the qualitative versus quantitative biomedical paradigm and suggested that “The integration of feminist intersectionality and the biomedical paradigm in research occurs in the selection of research problems, design, and methods, as well as the operationalization of the assumptions of each paradigm through the research process” (5,p.44). The contrast of biomedical and intersectional paradigms and their traditional affiliations with quantitative vs. qualitative methods reinforce a binary way of thinking that must be questioned and complemented from a philosophical perspective that embraces the complexity of health inequities.
In Bogota, the Territorial Health Model (THM) for the city has been built and adjusted under the leadership of the District’s Department of Health, and in accordance with the 2020-2024 District Development Plan. It seeks to implement strategies based on primary health care (PHC), with a sufficient, efficient and modern service infrastructure to serve the population of Bogota and, thus, reduce avoidable morbidity and mortality and improve their living conditions. In this sense, the THM proposes addressing the territory and realities of the communities, articulating collective and individual health care in a continuum and, at the same time, facilitating access to health care services for the most vulnerable population groups that require greater care in the capital of Colombia. The THM uses a differential approach and an intersectional approach, with the intent to incorporate the diversity of the city’s population groups, providing comprehensive care, protection, and guarantee of the rights of all citizens (6,7).
In the context of the implementation process of this model, the project titled Complemento al esquema de medición de avance del Modelo Territorial de Salud, basado en atención primaria en salud: Salud a mi Barrio/Salud a mi Vereda en Bogotá D.C., was carried out, which aimed to propose strategies for the monitoring, follow-up, and evaluation of the THM. This paper is written around this project and offers the definitions for the concepts of differential approach and intersectionality, based on a review of the literature and the narratives of the participants in the world café-style group interviews. It also specifies, within the differential approach, the definitions of disability, gender, and diverse sexual orientation. Thus, it seeks to provide information for the incorporation and implementation of the differential approach in comprehensive health care models.
Methodology
A multimethod strategy was developed, consisting of two phases: the first one, a literature search, in order to identify the definitions of intersectionality and differential approach, and the second one, based on a qualitative, world café-style methodology, in order to recognize the perspectives both of the people in the institutions and in non-institutional communities. These phases were developed through Special Cooperation Agreement No. 3028486 of 2021 between the District’s Department of Health of Bogota, D.C. (Colombia) and Pontificia Universidad Javeriana.
Literature review
Through a systematic literature search, by checking the PubMed, Elsevier, Biblioteca Virtual en Salud, Web of Science, and ProQuest platforms, in addition to a gray literature search through web search engines, web pages of governmental and non-governmental institutions, and after checking documents submitted by professionals from the District’s Department of Health of Bogotá D.C., the definitions of intersectionality and differential approach with emphasis on disability, gender, and diverse sexual orientation in the context of primary and community health care models were identified. Documents written in English, Spanish or Portuguese, published after the year 2000 and which provided the definitions of interest, were included. There were no restrictions by study design.
A search strategy was designed, consisting of controlled vocabulary (MeSH, Emtree, and DeCS) and free language. The strategy was adapted according to the thesaurus of each database searched. The terms used can be found in the supplementary material to this paper. Additional free and indexing terms were identified using the Vosviewer tool (8). The search was carried out in December 2021.
Duplicate documents were removed, after which two reviewers independently selected the publications to be included, based on titles and abstracts. The process was carried out using the Rayyan© (9) platform. A single evaluator read the selected papers in their entirety and proceeded to code the text of the articles to extract concepts and definitions using the NVivo 12® (10) program.
World Café
Qualitative data was then collected, using the world café-style group interview strategy. The purpose was to “discuss a particular topic in small conversation groups that rotate as the workshop unfolds” (11). This allows a more in-depth knowledge that contributes to the discussion of the central subject of debate and also makes it easier for the participants to propose different solutions and new proposals. This methodology consists of deliberations that are not subject to predetermined procedures and are carried out by a number of demographically diverse citizens. Eight group interviews were conducted, each consisting of two groups, one with officials from institutions and the other with participants from the community. Each world café-style group interview included participants from groups of interest to the project, framed within the differential approach.
Participant selection was based on convenience. Community participants were selected based on their membership in various groups, including women and men at different life stages, victims of armed conflict, peasants, LGBTIQ+ individuals, people with disabilities and their caregivers, migrants, and other vulnerable groups such as recyclers, paid sex workers, and street dwellers. Researchers reached out to these participants directly or through social and community leaders or organizations dedicated to these groups. The officials of the institutions were experts in the differential approach, the intersectional perspective, or the groups mentioned earlier. The profiles of the officials were diverse and belonged to different entities or institutions, including the district health secretary, health promotion companies, health service providers, foundations, and organizations.
The participants were assigned to groups for deliberation, and given the flexibility characteristic of this specific modality, the way was given to the progressive construction of new conversations, combining the discussion groups after a determined time (11). In this case, the groups came from the institutions and the community to exchange knowledge of what was dealt with in the first part. All participants completed a characterization survey before starting the interviews. The survey can be consulted in the supplementary material.
Community participants discussed their experiences, perspectives, and expectations concerning healthcare and the adjustments they believe are necessary to provide care to populations with multiple levels of inequality. The discussions allowed for the introduction of new topics and further deliberation. In the group of institutional officials, the adopted definitions of intersectionality and the differential approach were explored. A discussion was encouraged on implementing the approach in vulnerable populations and the challenges involved in its application to those with multiple levels of inequality (12,13).
Then, the pre-established and emerging categories of each of the group interviews were analyzed. Finally, an integrated definition of the differential approach, as well as of intersectionality, was consolidated as a result of a process of combining different data, known as triangulation, carried out by the researchers, taking into account the findings of the literature and the analyzes of the world café-style group interviews.
Ethical considerations
Approval was obtained from the Research and Institutional Ethics Committee of the School of Medicine of Pontificia Universidad Javeriana and Hospital Universitario San Ignacio on 28 September 2021, through Record No. 34/2021.
At the beginning of each world café, a verbal informed consent was shared with the participants, in which they were assured of confidentiality, anonymity, willingness, and other ethical considerations consistent with and defined in the qualitative research methods. Authorization was also requested to record the conversations through audio recordings and to collect the material resulting from the research.
Results
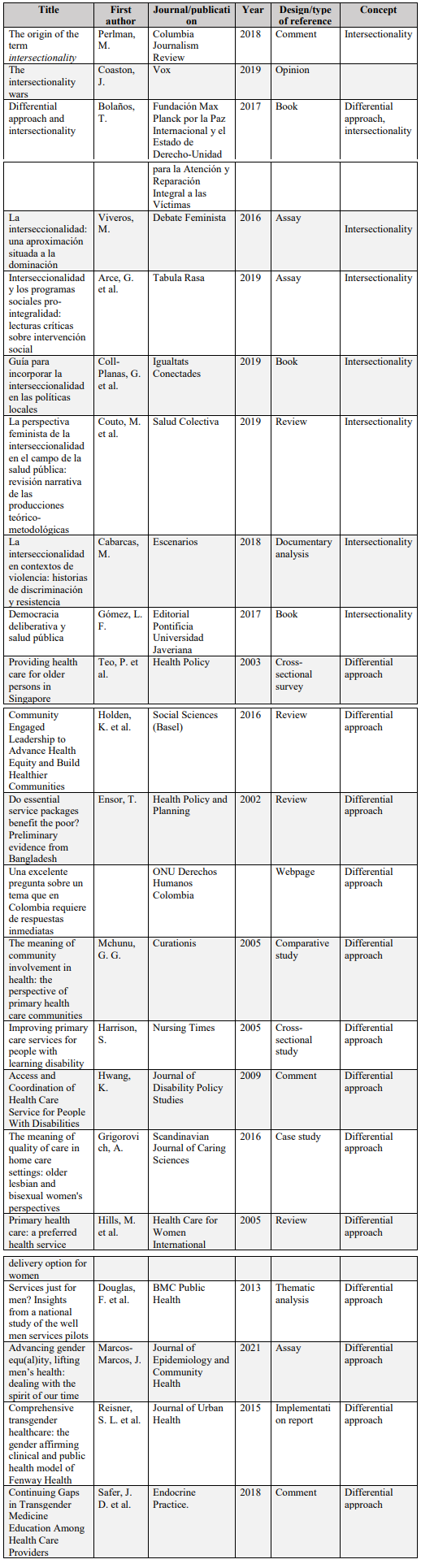
The search allowed us to identify 35 references with conceptual approaches or definitions for the differential approach or the intersectional perspective in comprehensive health care models. Thirteen of the identified references are operational documents or with guidelines from entities such as the Ministry of Health and Social Protection, the Departments of Health (Bogota and Medellin), the Governor’s Office of Antioquia, the Colombian Family Welfare Institute and the United Nations Organization (14). These references are detailed in Table 1. The remaining 22 references are described in Table 2.
Table 1
Operational documents or institutional guidelines included in the review
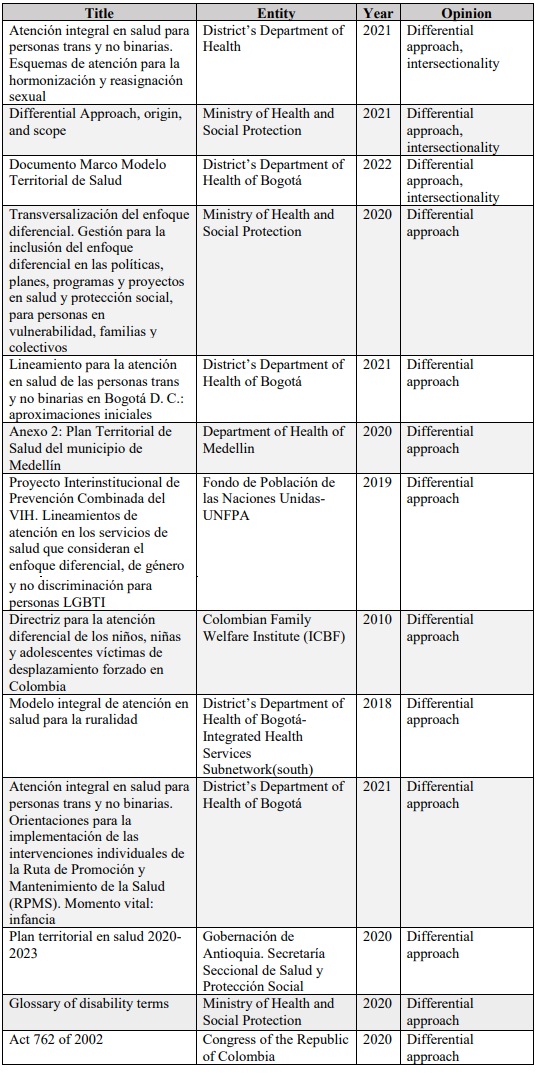
Table 2
Characteristics of the documents included in the literature review
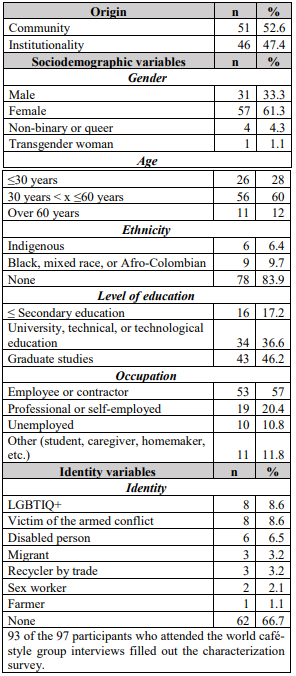
Eight world café-style group interviews were conducted, in which a total of 97 people participated. Table 3 characterizes the participants in these group interviews.
Table 3
Characterization of participants in the world café-style group interviews
The Differential Approach
It is a cultural and historical construct that is structured from the human rights approach, in which the principles of non-discrimination, social inclusion and human dignity are appealed to (15,16). Based on the human rights approach, the differential approach seeks to claim and legitimate differences (17), understanding that the populations to be described have experienced historical exclusion, which makes the differential approach an ethical imperative (15).
The descriptions, in terms of the object of the differential approach, are aimed at the need to recognize groups, populations, or collectives with special characteristics as subjects of rights, capable of holding institutions, the State, and society, in general, responsible for generating differential responses that meet the specific needs of these populations and achieve a greater well-being for them (15,16). Another object of the approach is to achieve a state of equality and guarantee of rights for differential populations, that is, to seek equity in the right to difference (15-20).
When describing these vulnerable populations, some authors do so as persons, groups, or collectives that are in or at risk of vulnerability, manifest violation, marginality, unequal treatment, discrimination, disadvantage, or exclusion (15,17,19). With respect to specific population groups, the following are recognized: people with disabilities, farmers, social leaders, indigenous people, Afro-descendants, victims of violence, victims of forced displacement, human rights defenders, members of trade union organizations or LGBTIQ+ groups, as well as all those that are not mentioned, but who, due to their cultural, ethnic, gender, sexual orientation, economic, social, physical or mental conditions, are in a vulnerable situation (15,17-19,21-23).
Three functions or components of the differential approach were identified: first, the differential approach as a method of analysis, where the entire process of identification and recognition of the situations and risks of specific populations takes place (15,24,25). Second, the differential approach as a guide to action, where the differential actions to meet the objectives of the approach are generated (15,24-26). Third, the differential approach as a method of evaluating the institutional and community response (15,27). Based on the above, the following definition for differential population is suggested: specific population groups who are in a situation or condition of vulnerability and, therefore, require a particular institutional response.
Differential approach for people with disabilities
The findings in the literature about the description of the differential approach for people with disabilities focused mainly on children with learning disabilities. This differential approach must have the capacity to support healthy decisions, based on adequate and accessible information, that improve the lifestyle of this population (28). It is also essential that an approach be made that understands that functionality does not depend exclusively on the disability, but that it is affected by other conditions such as gender, age, race, or socioeconomic level, as well as by social, economic factors, and environmental factors exogenous to the subject (28,29).
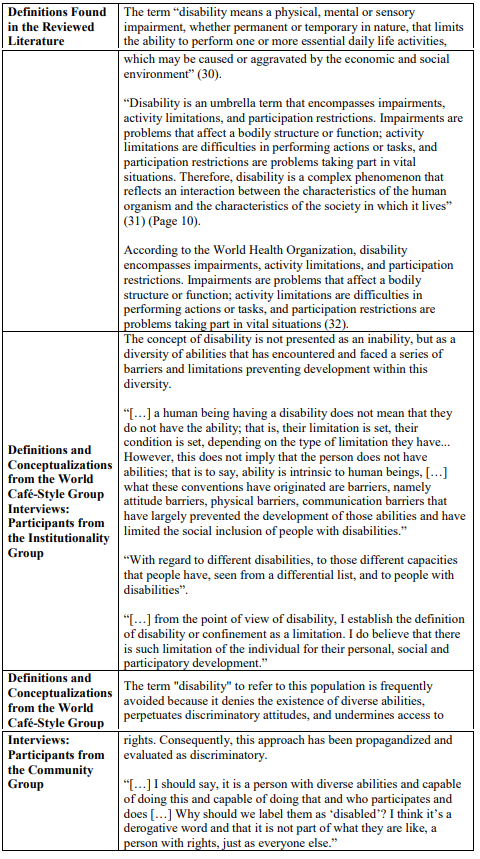
Table 4 presents the findings of the reviewed literature and the conceptualizations made by the participants in the world café on disability (people with disabilities, caregivers and institutional representatives) convened.
Table 4
Synthesis of findings around the concept of disability
The differential approach for people with disabilities should favor the coordination of medical care and community support, such as to minimize the influence of those exogenous or endogenous factors and allow all individuals to receive the necessary services to maximize the enjoyment of a normal, age-appropriate functional status (described as not dying or becoming prematurely disabled). This coordination allows the engagement of primary care professionals in the care of these patients, without leaving said care exclusively in the hands of specialist medical and psychosocial groups (28,29).
Participants of the world café-style group interviews believe that recognizing particular characteristics implies accepting differences that lead to different health risks and, therefore, to different requirements in terms of health care. In particular, recognition of the disabled population as people with their own abilities and the right to comprehensive access to health care, recovery, and rehabilitation, is proposed (see Table 4).
Considering the summary of the findings in the literature and in the world café, we propose the following definition for the differential approach regarding people with disabilities:
The differential approach for people with disabilities seeks to overcome social and contextual barriers to guarantee the effective enjoyment of the rights of the population in a situation or condition of disability. It is defined as the population with a situation or condition generated from the relationship between the person, society, and the context in which they live, which limits the full and effective participation of the individual in society under equal conditions, as well as their performance and development.
Gender and diverse sexual orientation approach
Gender is part of the differential approach, as it is a social determinant that regulates human relations (20). It is considered a category of analysis that facilitates a holistic understanding of society, economy, history, politics, among other variables. At the same time, it facilitates the understanding of the social and cultural construction of gender-related stereotypes and highlights the quality of the relationships woven between women, men, gays, bisexuals, lesbians, transsexuals, intersexuals, cross-dressers, transvestites, and other diverse sexual orientations (20).
Recognition of both biological differences and gender identities is required, as they directly influence the health-disease processes experienced by the populations. Therefore, health care services should focus on differentiated and specific care measures (15).
The term LGTBIQ+ has two components: one related to gender identity and the other one alluding to a political dialogue strategy. The acronym LGTBIQ+ brings together the social and political confluence of lesbian, gay, transgender, bisexual, intersex, and queer people and includes other sexual identities, with the aim of positioning their inclusion and social recognition on the political agenda (17).
Table 5 presents the results of the definitions around the concepts of gender and diverse sexual orientation found in the literature review, as well as in the narratives of the institutional participants of the world café-style group interviews.
Table 5
Summary of findings about the concept of gender and diverse sexual orientation approach
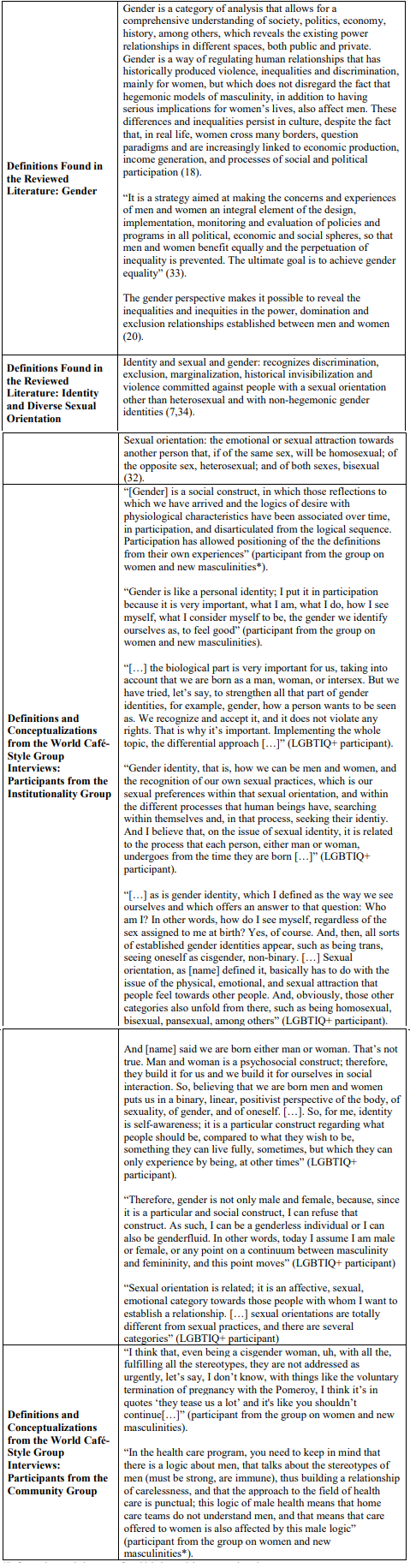
*Refers to the population group for which the participant was selected.
Regarding the provision of health care services, according to some studies, there are strategies that contribute to generating more empathic relationships with people from the LGBTIQ+ community: for example, including their preferred name, pronouns, assigned sex at birth, and gender identity in their clinical records. This would allow us to know more about the patient and provide higher quality care (35).
Participants from the community group in the world café-style group interviews focused on the importance of treating people with diverse sexual orientations with care and respect, recognizing the different vulnerabilities to which they are exposed. Lesbian and bisexual women, for their part, believe that health care professionals should be trained on how to treat them, since they are afraid of being rejected, judged, mistreated and disrespected due to their life situation. Having prior knowledge about the different sexual orientations and gender identities will help to understand their experiences and be tolerant (36,37).
Based on the summary and analysis of the definitions found in the literature, as well as the explicit and implicit narratives of the participants in the world cafés, we propose the following definitions of gender approach and diverse sexual orientation:
The gender approach is based on understanding that it is a social and cultural construct based on sexual differences that assigns representations of what is feminine and what is masculine and which is instituted on the unequal allocation of resources, power, and the subordination of femininity. In this sense, the inequalities between men and women, and between the different masculinities and femininities, are revealed, which allows differences and discrimination to be interpreted, providing elements of analysis on the forms of distribution of power.
According to the diverse gender identities and sexual orientations approach, gender is a social and cultural construct that has historically been limited to binarity as a power structure, that has ignored, on the one hand, the internal and individual experiences of gender and, on the other, sexual orientation as an emotional and physical category towards those people with whom one wishes to have an intimate relationship. Recognizing and acceping these differences, which resignify and go beyond binarity, favor the effective enforcement of rights and prevent inequalities and discrimination.
Intersectionality
The origin of the term intersectionality has been attributed to Kimberlé W. Crenshaw, who coined it in 1989 from the discussion about the discrimination suffered by women of African descent, where he indicated that they were much more than the simple sum of sexism and racism (24,38,39). In this sense, intersectionality is also seen as a critique of the lack of cohesion between feminism and black activism (38,39). Later, in 2015, and based on Crenshaw’s ideas, the Oxford English Dictionary identified it as a theoretical approach based on the interconnection of social categories such as race, social class, and gender, which create complex systems of discrimination or disadvantage (38,39).
Table 6 presents the results regarding the definitions of the concept of intersectionality found in the reviewed literature, as well as the conceptualizations of the participants in the world café-style group interviews.
Table 6
Synthesis of findings around the concept of intersectionality

*Refers to the population group for which the participant was selected.
Intersectionality allows us to understand the health-disease processes and the consequent inequity in health that happens around different oppressions in a given historical, social and cultural context. It implies understanding that the different particularities that have been instruments of domination are interrelated and that they affect the subject jointly, and, therefore, a rigid categorization of differential conditions or situations is inadequate. This implies that, in the field of public policy, the approach proposes a complex approach that allows understanding and acting on the profound interaction between the axes of inequality (24,26,42,43).
As in the differential approach, the intersectional approach recognizes these oppressions as historical. These two approaches complement each other, as both are tools that facilitate the conception and execution of public policies with an emphasis on the most vulnerable population. The relationship is also present with the human rights approach, and therefore the intersectional approach requires comprehensive care based on the protection, promotion and defense of human rights, taking into account the multiple vulnerabilities that have already been described (24,44,45).
According to the findings of the world cafés, intersectionality is strongly linked to the differential approach. Participants agree that the convergence of several situations in the same individual is a fundamental aspect of intersectionality. Table 6 includes details on the interviews. Based on the analysis of the different sources of information and using an iterative consensus process, we propose the following conceptual definition:
Intersectionality constitutes a perspective that seeks to identify and understand how multiple conditions, situations or characteristics intertwine that make up a complex system of oppressive structures that lead to simultaneous vulnerabilities. This approach does not seek to rank or add the axes of oppression; on the contrary, it establishes a network configuration of structured social positions.
Discussion and conclusions
According to the reviewed literature, the differential approach and the intersectional perspective are complementary categories that differ in how discrimination is understood and addressed, starting from a joint base. Unlike the findings in the literature review, there is ambiguity between the concepts among the participating users and institutions, since they assume that intersectionality comprises the sum of differential situations in the same subject. Regarding the comprehensive health care models, based on a human rights approach, and based on the information collected, it is evident that vulnerability and discrimination must be considered at the level of the differential approach and the intersectional perspective.
From the differential approach, comprehensive health care models should see to each of the differential populations, understanding that their health needs and risks differ. On the other hand, those individuals who are going through more than one situation of vulnerability should be taken into consideration, as it would be inequitable to offer them services for each of the “boxes” they belong to, becuase it further increases their vulnerabilities and possibly forces them to a series of unnecessary paperwork and procedures.
Faced with people going through various situations of vulnerability at the same time, the intersectional perspective promotes a comprehensive approach to the individual. To illustrate: for a lesbian, adolescent woman of low socioeconomic level, four situations should not be considered; she must be approached as a whole, understanding that her context generates risks and challenges for health care systems, which are so particular that four different approaches would not be able to respond holistically to their health needs.
According to the insights gathered from the interviews, the community recognizes the importance of thoroughly characterizing the population to determine their unique needs. This information is crucial in allocating resources, setting priorities, and developing comprehensive healthcare plans. In addition, incorporating this consideration in designing, implementing, and evaluating a differentiated approach in holistic healthcare models is essential for their success.
Also, to this date, the recognition of the role of social determinants in the generation of inequities in health has not managed to translate into interventions that improve the disparate health outcomes between populations and between individuals. It is necessary to broaden the understanding of the dynamics that generate health inequalities and the resources to research them. This research shows the complexity of the social forces that generate inequalities, and, although it provides flexibility from the methodology to approach the definitions of interest, it also raises the concern about which aspects were not considered in the final analysis due to the chosen avenues of research. Finally, although the data collection, synthesis and analysis methods were rigorous, obstacles were found in terms of interpreting and translating complex knowledge and contexts into condensed and accessible messages for the formulation of action plans of a healthcare model with the intersectionality approach and the differential approach.
Ultimately, every intervention in the healthcare field must have an adequate conceptualization of the differential approaches and the intersectional perspective so that, first of all, it serves to analyze the realities of the different forms of discrimination of vulnerable populations and, second of all, it takes into account the analysis of these realities to provide adequate health care and protection of the rights of these populations. Clarity in these concepts will make it easier for interventions in the healthcare field to have the capacity to respond to the differences of certain populations, to offer timely, quality care adapted to the needs of each individual.
Future work may delver further into the conceptualization and implementation of other approaches, such as the differential ethnic approach. It will also be pertinent to delve further into the differential approach, emphasizing on the new masculinities, where the vulnerability of men and their needs in terms of health are recognized, in order to jointly build better strategies for the promotion and care of male health, free of stereotypes and stigmas, which not only violate women’s access to health care, but also limit men in their self-care and mutual health care.
Funding
This research was developed under Special Cooperation Agreement No. 1950482 for the Promotion of Scientific and Technological Activities between the District’s Department of Health and Pontificia Universidad Javeriana (Bogota, Colombia). The funds linked to the special cooperation agreement come from the District Health Financial Fund.
Conflict of interest
Authors declare not to have any conflict of interest.
Acknowledgments
We would like to thank the members of the community, the specialists from the District’s Department of Health, the Social Integration Department, the Colombian Family Welfare Institute Capital Salud EPS-S, Javesalud IPS, Organización ACDI/VOCA, Corporación Casa de la Mujer Suba, Colectivo Hombres y Masculinidades, Grupo Stonewall, Consejo de Discapacidad de Chapinero, Fundación Saldarriaga Concha, Fundación Mahuanpi, Fundación Red Somos, Fundación Zarakua, Equipo de Justicia y Paz de las Hermanas de la Caridad del Buen Pastor, and Entidad Medioambiental de Recicladores, who supported us in the development of the world cafés.
We would also like to thank the work team of the Home Care Teams fromthe District’s Department of Health for their logistical and technical support in carrying out this research. Finally, we would like to thank Viviana Rodríguez for coordinating the project and for her comments on the final version of the manuscript.
References
1. Commission on Social Determinants of Health. Final report of the commission on social determinants of health. Closing the gap in a generation: health equity through action on the social determinants of health. Geneva: World Health Organization; 2008.
2. Institute of Medicine (US) Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care. Unequal treatment: confronting racial and ethnic disparities in health care. Washington (DC): National Academies Press (US); 2003.
3. Centers for Disease Control and Prevention. Establishing a holistic framework to reduce inequities in HIV, Viral hepatitis, STDs, and tuberculosis in the United States. Atlanta (GA): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; October 2010.
4. Mullings L, Schulz AJ. Intersectionality and health: an introduction. In: Gender, race, class, & health: intersectional approaches. Hoboken, NJ, US: Jossey-Bass/Wiley; 2006. p. 3–17.
5. Kelly UA. Integrating intersectionality and biomedicine in health disparities research. ANS Adv Nurs Sci. 2009;32(2):E42–56.
6. Alcaldía Mayor de Bogotá D.C, Secretaría de Planeación, Consejo de Bogotá D.C. Plan Distrital de Desarrollo 2020-2024 Un Nuevo Contrato Social y Ambiental para la Bogotá del Siglo XXI. Bogotá; 2020 Jun.
7. Secretaría Distrital de Salud de Bogotá. Documento marco modelo territorial de salud. Bogotá; 2022 Mar.
8. Eck N, Waltman L. VOSViewer. Netherlands: 27 January 2020; 2020.
9. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Systematic Reviews. 2016 Dec 5;5(1):210.
10. QSR International Pty Ltd. NVivo (Version 12). 2018.
11. Löhr K, Weinhardt M, Sieber S. The “World Café” as a participatory method for collecting qualitative data. Int J Qual Meth. 2020 Jan 1;19.
12. Gutiérrez LF. Democracia deliberativa y salud pública. Bogotá: Pontificia Universidad Javeriana; 2017.
13. Gabriela Panozzo Zenere A, Nacional de Rosario U. Quiénes son los visitantes de los museos de arte. Particularidades de los públicos del fin de semana en el Museo de Arte de Tigre (Argentina). Anais do Museu Paulista: História e Cultura Material. 2020 Jun 10;28.
14. Pontificia Universidad Javeriana. Segunda evidencia: documento de informe sobre el análisis de las definiciones de los enfoques del MTS. Bogotá; 2022 Apr (Convenio Especial de Cooperación 3028486 de 2021: Complemento del esquema de medición de avance del Modelo Territorial de Salud, basado en atención primaria en salud en Bogotá D.C.: Salud a mi Barrio, Salud a mi Vereda).
15. Ministerio de Salud y Protección Social. Enfoque diferencial origen y alcances; 2021.
16. Ministerio de Salud y Protección Social. Transversalización del enfoque diferencial: gestión para la inclusión del enfoque diferencial en las políticas, planes, programas y proyectos en salud y protección social, para personas en vulnerabilidad, familias y colectivos. 2020 Jul. Report No.: ASIF02 Versión 2.
17. Secretaría Distrital de Salud de Bogotá. Lineamiento para la atención en salud de las personas trans y no binarias en Bogotá D.C: aproximaciones iniciales. Bogotá; 2021.
18. Secretaría de Salud de Medellín. Anexo 2: Plan territorial de salud del municipio de Medellín; 2020.
19. Gobernación de Antioquia. Secretaría seccional de salud y protección social. Plan territorial en salud 2020-2023; 2020.
20. Fondo de Población de las Naciones Unidas (UNFPA). Proyecto Interinstitucional de Prevención Combinada del VIH: lineamientos de atención en los servicios de salud que consideran el enfoque diferencial, de género y no discriminación para personas LGBTI. Bogotá; 2019.
21. Teo P, Chan A, Straughan P. Providing health care for older persons in Singapore. Health Policy. 2003;64(3):399–413.
22. Holden K, Akintobi T, Hopkins J, Belton A, McGregor B, Blanks S, et al. Community engaged leadership to advance health equity and build healthier communities. Soc Sci. 2016;5(1):2–2.
23. Ensor T, Dave-Sen P, Ali L, Hossain A, Begum SA, Moral H. Do essential service packages benefit the poor? Preliminary evidence from Bangladesh. Health Policy and Planning. 2002;17(3):247–247.
24. Bolaños T, Filisi I. Enfoque diferencial e interseccional. Bogotá; 2017 Nov.
25. ONU Derechos Humanos Colombia. Una excelente pregunta sobre un tema que en Colombia requiere de respuestas inmediatas. [Internet]. [Cited 2022 Feb 21]. Available from: https://www.hchr.org.co/index.php/76-boletin/recursos/2470-ique-es-elenfoque-diferencial
26. Secretaría Distrital de Salud de Bogotá. Atención integral en salud para personas trans y no binarias. Esquemas de atención para la hormonización y reasignación sexual. Bogotá; 2021.
27. Colombian Family Welfare Institute (ICBF). Directriz para la atención diferencial de los niños, niñas y adolescentes víctimas de desplazamiento forzado en Colombia. 2010.
28. Harrison S, Berry L. Improving primary care services for people with learning disability. Nurs Times. 2005;101(1):38–40.
29. Hwang K, Johnston M, Tulsky D, Wood K, Dyson-Hudson T, Komaroff E. Access and coordination of health care service for people with disabilities. J Disab Policy Stud. 2009;20(1):28–34.
30. Congreso de la República de Colombia. Act 762 of 2002; 2002.
31. Ministerio de Salud y Protección Social. Oficina de Promoción Social. Grupo de Gestión en Discapacidad. Glosario de términos sobre discapacidad; 2020.
32. Secretaría Distrital de Salud de Bogotá. Guía para la apropiación e implementación del enfoque poblacional, diferencial y de género. 2021. Bogotá; 2021.
33. Consejo Económico y Social. Decisiones adoptadas por el Consejo Económico y Social en su periodo de sesiones organización de 1997; 1997.
34. Departamento Nacional de Planeación. Plan Nacional de Desarrollo 2010-2014. Bogotá; 2010.
35. Reisner SL, Bradford J, Hopwood R, Gonzalez A, Makadon H, Todisco D, et al. Comprehensive transgender healthcare: the gender affirming clinical and public health model of Fenway Health. J Urban Health. 2015 Jun 5;92(3):584–92.
36. Grigorovich A. The meaning of quality of care in home care settings: older lesbian and bisexual women’s perspectives. Scand J Caring Sci. 2016;30(1):108–16.
37. Safer JD. Continuing gaps in transgender medicine education among health care providers. Endocrine Practice. 2018 Dec 1;24(12):1106–7.
38. Perlman M. The origin of the term ‘intersectionality’ - Columbia Journalism Review [Internet]. 2018 [cited 2022 Feb 22]. Available from: https://www.cjr.org/language_corner/intersectionality.php
39. Coaston J. The intersectionality wars [Internet]. 2019 [cited 2022 Feb 22]. Available from: https://www.vox.com/the-highlight/2019/5/20/18542843/intersectionality-conservatism-law-race-gender-discrimination
40. Coll-Planas G, Solà-Morales R. Guía para incorporar la interseccionalidad en las políticas locales. Comisión Europea; 2019.
41. Couto MT, de Oliveira E, Alves Separavich MA, Luiz ODC. La perspectiva feminista de la interseccionalidad en el campo de la salud pública: revisión narrativa de las producciones teórico-metodológicas. Salud Colectiva. 2019 Mar 9;15:e1994.
42. Viveros Vigoya M. La interseccionalidad: una aproximación situada a la dominación. Debate Feminista. 2016 Oct 1;52:1–17.
43. Arce GM, Larraín-Salas D. Interseccionalidad y los programas sociales pro-integralidad: lecturas críticas sobre intervención social. Tabula Rasa. 2019;(30). https://doi.org/10.25058/20112742.n30.08
44. Secretaría Distrital de Salud de Bogotá. Atención integral en salud para personas trans y no binarias: orientaciones para la implementación de las intervenciones individuales de la Ruta de Promoción y Mantenimiento de la Salud (RPMS). Momento vital: Infancia. Bogotá; 2021.
45. Cabarcas Rivera MA. La interseccionalidad en contextos de violencia: historias de discriminación y resistencia. Escenarios. 2018;16(1):47–53.
Author notes
* Departamento de Epidemiología Clínica y Bioestadística, Facultad de Medicina, Pontificia Universidad Javeriana, Bogotá, Colombia. Universidad Nacional de Colombia.
** Departamento de Epidemiología Clínica y Bioestadística, Facultad de Medicina, Pontificia Universidad Javeriana, Bogotá, Colombia. Fundación Universitaria Sanitas.
a Correspondence author: isabel.moreno@javeriana.edu.co
Additional information
How to cite: Marín Urrego JC, Moreno Luna S, Peña Torres E, Mariño J, Martínez-Álvarez E, Duque Yara N, Cadena Camargo Y. Defining differential approach and intersectional perspective: a multimethod study. Univ. Med. 2023;64(1) https://doi.org/10.11144/Javeriana.umed64-1.edpi









