








APA
ISO 690-2
Harvard
Haga clic en un formato de citación
Design and Validation of Instruments to assess Knowledge, Self-efficacy, and Complications in Home Tracheostomy Care
Diseño y validación de instrumentos para evaluar conocimiento, autoeficacia y complicaciones en traqueostomía domiciliaria
Desenho e validação de instrumentos para avaliar o conhecimento, a autoeficácia e as complicações no cuidado domiciliar de traqueostomia
Edith Periañez López ![]() , María Guadalupe MorenoMonsiváis
, María Guadalupe MorenoMonsiváis ![]()
Design and Validation of Instruments to assess Knowledge, Self-efficacy, and Complications in Home Tracheostomy Care
Universitas Médica, vol. 67, 2026
Pontificia Universidad Javeriana
Edith Periañez López a edith.perianezl@uanl.edu.mx
Universidad Autónoma de Nuevo León, Monterrey, México
María Guadalupe MorenoMonsiváis
Universidad Autónoma de Nuevo León, Monterrey, México
Received: 12 august 2025
Accepted: 15 august 2025
Abstract: Introduction: Home-based care of adults with tracheostomy requires family caregivers to develop technical knowledge, clinical skills, and adequate levels of self-efficacy in order to prevent and detect complications associated with the procedure. Objective: To design and obtain the Content Validity Coefficient (CVC) of two questionnaires: one assessing knowledge related to home tracheostomy care and another assessing self-efficacy for tracheostomy management. In addition, to develop and validate two clinical rubrics to identify early and late complications in individuals with tracheostomy. Materials and methods: A methodological study developed in three phases: a literature review to identify conceptual and clinical content, the design and construction of the questionnaires and rubrics, and content validation using the CVC to evaluate the clarity, relevance, and pertinence of the developed instruments. Results: Both the questionnaires and the rubrics achieved CVC values greater than 0.90, which, according to the applied methodology, indicate excellent levels of validity and agreement. Conclusions: The developed instruments represent a significant contribution to both education and the assessment of knowledge and self-efficacy related to home tracheostomy care among family caregivers, as well as to the identification of complications in individuals with tracheostomy through the use of clinical rubrics.
Keywords:caregivers, tracheostomy, knowledge, self-efficacy, nursing, validation study.
Resumen: Introducción: El cuidado domiciliario de personas adultas con traqueostomía requiere que los cuidadores familiares desarrollen conocimientos técnicos, habilidades clínicas y una adecuada autoeficacia para prevenir y detectar complicaciones asociadas con el procedimiento. Objetivo: Diseñar y obtener el coeficiente de validez de contenido (CVC) de dos cuestionarios, uno de conocimientos sobre el manejo de la traqueostomía en el domicilio y otro de autoeficacia para su manejo. Asimismo, de dos rúbricas clínicas para identificar complicaciones precoces y tardías en personas con traqueostomía. Material y métodos: Estudio metodológico desarrollado en tres fases: una revisión bibliográfica para la identificación de contenidos conceptuales y clínicos, el diseño y construcción de los cuestionarios y rúbricas, y la validación de contenido mediante el CVC para evaluar claridad, pertinencia y relevancia de los instrumentos elaborados. Resultados: Tanto los cuestionarios como las rúbricas obtuvieron un CVC superior a 0,90 que, de acuerdo con la metodología utilizada, tienen validez y concordancia excelentes. Conclusiones: Los instrumentos diseñados representan una contribución significativa tanto para la educación como para la evaluación de conocimientos y autoeficacia para el manejo de traqueostomía en domicilio por cuidadores familiares, así como para la identificación de complicaciones en personas con traqueostomía, mediante las rúbricas clínicas.
Palabras clave: cuidadores, traqueostomía, conocimiento, autoeficacia, enfermería, estudio de validación.
Resumo: Introdução: O cuidado domiciliar de pessoas adultas com traqueostomia requer que os cuidadores familiares desenvolvam conhecimentos técnicos, habilidades clínicas e níveis adequados de autoeficácia para prevenir e identificar complicações associadas ao procedimento. Objetivo: Desenhar e obter o coeficiente de validade de conteúdo (CVC) de dois questionários: um para avaliar o conhecimento sobre o manejo domiciliar da traqueostomia e outro para avaliar a autoeficácia para esse manejo. Além disso, desenvolver e validar duas rubricas clínicas para identificar complicações precoces e tardias em pessoas com traqueostomia. Materiais e métodos: Estudo metodológico desenvolvido em três fases: revisão da literatura para identificação de conteúdos conceituais e clínicos, elaboração e construção dos questionários e rubricas, e validação de conteúdo por meio do CVC para avaliar a clareza, pertinência e relevância dos instrumentos desenvolvidos. Resultados: Tanto os questionários quanto as rubricas apresentaram valores de CVC superiores a 0,90, o que, de acordo com a metodologia utilizada, indica níveis excelentes de validade e concordância. Conclusões: Os instrumentos desenvolvidos representam uma contribuição significativa tanto para a educação quanto para a avaliação do conhecimento e da autoeficácia no manejo domiciliar da traqueostomia por cuidadores familiares, assim como para a identificação de complicações em pessoas com traqueostomia por meio das rubricas clínicas.
Palavras-chave: cuidadores, traqueostomia, conhecimento, autoeficácia, enfermagem, estudo de validação.
Introduction
Home care of adults with a tracheostomy places a substantial burden on family members, as it encompasses emotional, educational, social, and structural domains. One of the main challenges is emotional overload, which includes anxiety, fear, and uncertainty regarding the responsibility of tracheostomy management, particularly during the transition period from hospital to home (1–4).
Likewise, deficiencies have been identified in the education provided to caregivers for tracheostomy management, which is often insufficient to address complex situations such as emergencies or specific techniques such as tracheal suctioning. This affects perceived confidence and safety when assuming care (5,6).
Other relevant challenges include difficulties in accessing and coordinating resources, such as obtaining medical supplies or support from home nursing services, compounded by the lack of standardization in care (5,7). The caregiving experience itself also affects quality of life and family functioning, as it disrupts sleep, limits social and work life, and creates isolation (2,3). Added to this is a perception of limited professional and social support, especially after hospital discharge (1,7,8).
Training caregivers of persons with a tracheostomy improves their knowledge, confidence, and skills to manage equipment, which can help reduce complications and enables a safer transition to the home (9,10). Standardized programs have been shown to reduce adverse events, such as infections and hospital readmissions (11). Some clinical guidelines recommend including hands-on training and validating skills to promote a safe home environment (12,13).
From a psychosocial perspective, caregiver self-efficacy is a central construct grounded in Bandura’s social cognitive theory (14) and refers to the perceived capability to perform specific behaviors in demanding situations. In the context of home tracheostomy care, adequate self-efficacy is associated with greater adherence to care and better performance of procedures (15).
On the other hand, regarding complications that most frequently occur at home, tube obstruction, accidental displacement, local and respiratory infections, and device malfunction have been described, and to a lesser extent, bleeding and complications related to tracheal structure (16,17). Having a rubric to assess potential complications that an adult with a tracheostomy may develop would help caregivers identify them in a timely manner.
In the literature review for this study, no validated instruments were identified to structurally assess caregivers’ knowledge and self-efficacy for performing specific procedures. These include oral and tracheostomy secretion suctioning, proper cleaning of materials, cleaning of the tracheostomy tube and inner cannula, stoma care, recannulation after accidental decannulation, and identification of complications.
Therefore, the aim of this study is to design and obtain the content validity coefficient (CVC) of two questionnaires—one assessing knowledge of home tracheostomy management and the other assessing self-efficacy for its management—as well as two clinical rubrics to identify early and late complications in persons with a tracheostomy.
These instruments constitute a tool for the training, monitoring, and evaluation of professional caregivers or family caregivers of adults with a tracheostomy. Likewise, they are useful tools for planning personalized educational interventions.
Materials and Methods
Study Type, Setting, and Period
A methodological study was conducted, divided into three phases. The first phase involved a literature review on tracheostomy management, whose evidence formed the basis for the initial design of the questionnaires and rubrics. In the second phase, the questionnaires and clinical rubrics were designed and developed, considering methodological guidelines for instrument creation and observable criteria for clinical performance.
In the third phase, content validity was assessed using the Content Validity Coefficient (CVC) proposed by Hernández-Nieto (18), based on the evaluation by a panel of nursing experts. The experts assessed each item in terms of clarity, relevance, coherence, and appropriateness using a Likert-type scale. Subsequently, the necessary adjustments were made based on the feedback received.
The validation process took place between November 2024 and June 2025 through virtual communication (email and WhatsApp). This stage did not involve direct participation from patients or caregivers, as the goal was solely to obtain the CVC through expert judgment.
Participants (Expert Panel)
A non-probability intentional sample of 20 experts was selected using the snowball sampling method, representing three areas: hospital practice, home care, and teaching.
Inclusion Criteria
Minimum of one year of experience in critical patient care, home care, or teaching.
Experience in the management of patients with a tracheostomy.
Prior participation in instrument validation processes.
Availability to participate in two rounds of evaluation.
Each instrument was evaluated by an independent panel consisting of between 7 and 10 experts, who participated in two successive rounds of validation.
Phase 1. Literature Review
The narrative literature review was based on scientific databases (PubMed, Scopus, SciELO, and Google Scholar), using descriptors related to tracheostomy care, nursing interventions, and home care, in both Spanish and English. Studies published between 2014 and 2024 were included. The findings helped define the conceptual and clinical content that underpinned the design of the instruments.
Phase 2. Construction of the Instruments
Four instruments were designed, grouped into two questionnaires and two clinical rubrics, which were developed independently due to their conceptual and operational differences.
Knowledge Questionnaire
A structured questionnaire was designed, consisting of 29 closed-ended multiple-choice questions (A, B, and C) focused on home tracheostomy management, divided into five thematic areas: secretion aspiration, cleaning of the tube and inner cannula, stoma care, reinsertion of the cannula after accidental decannulation, and identification of complications. The initial version of the instrument included 35 items, which were refined to the final version containing 29 items.
Self-Efficacy Questionnaire
A self-efficacy questionnaire was developed with 16 statements using a five-point Likert scale, aimed at assessing the caregiver's perceived confidence in performing procedures related to tracheostomy (19). This questionnaire was adjusted from 20 to 16 items.
Both questionnaires were designed for self-administration (20), considering their future application with caregivers.
Questionnaire Development Procedure
The methodological guidelines proposed by Martín Arribas (21) were followed, considering the following steps:
Definition of the construct and purpose.
Item formulation aligned with the educational objectives of the program.
Bias prevention through clear language, elimination of technical jargon, and non-leading item formulation.
Coding and scoring:
Knowledge: correct answers = 1 point; incorrect answers = 0 points; maximum score: 29.
Self-efficacy: Likert scale from 1 to 5; maximum score: 80.
The content of both instruments was based on scientific literature and specialized clinical guidelines (13,22–34)
Construction of the Clinical Rubrics
Two analytical rubrics were developed aimed at identifying complications associated with tracheostomy:
Early Complications Rubric: 6 clinical criteria assessed during the first week following the procedure.
Late Complications Rubric: 10 clinical criteria assessed from the seventh day onwar.
Both use a five-level performance scale (excellent, good, fair, poor, and very poor).
Procedure for Developing the Rubrics
The clinical rubrics were designed based on the methodological model proposed by Gatica-Lara and Uribarren-Berrueta (35). Initially, relevant clinical categories related to early and late complications of tracheostomy were identified from clinical guidelines and specialized literature (22,27,28). Subsequently, observable indicators and performance descriptors were defined for each category to establish objective clinical evaluation criteria.
Once the criteria and performance levels were defined, scores were assigned to each rubric, establishing a maximum score of 24 points for early complications and 40 points for late complications.
The early complications rubric was reduced from 7 to 6 criteria, while the late complications rubric remained with 10 criteria in its final version. Finally, interpretation ranges were defined to classify the clinical status of the tracheostomy into five levels: excellent, good, fair, poor, and very poor.
Phase 3. Content Validation by Experts
Only the content of the instruments was validated through expert judgment, following the method proposed by Hernández-Nieto (18). The participation of patients and caregivers was not included in this phase, as the objective of this study was to evaluate the theoretical and clinical relevance of the instruments. The empirical validation and application in the target population will be part of a subsequent independent study. The experts evaluated each item using a five-point Likert scale, considering the criteria of clarity, coherence, and relevance.
The process was carried out in two successive rounds of evaluation. The data were organized by rounds, coded with consecutive file numbers, and consolidated into a database for statistical analysis. The CVC was calculated for each item and globally, retaining only those items that reached a minimum acceptable value of 0.80.
Consideraciones éticas
Informed consent was obtained from all participating experts, and the study was conducted in accordance with the principles of the Declaration of Helsinki, respecting confidentiality and voluntary participation. No participation from patients or caregivers was included, as the aim was solely to obtain the CVC of the instruments through expert judgment.
Results
The results of the design and the CVC of the knowledge and self-efficacy questionnaires for home tracheostomy management, as well as the two clinical rubrics for identifying early and late complications in individuals with tracheostomies, are presented (Tables 1 and 2).
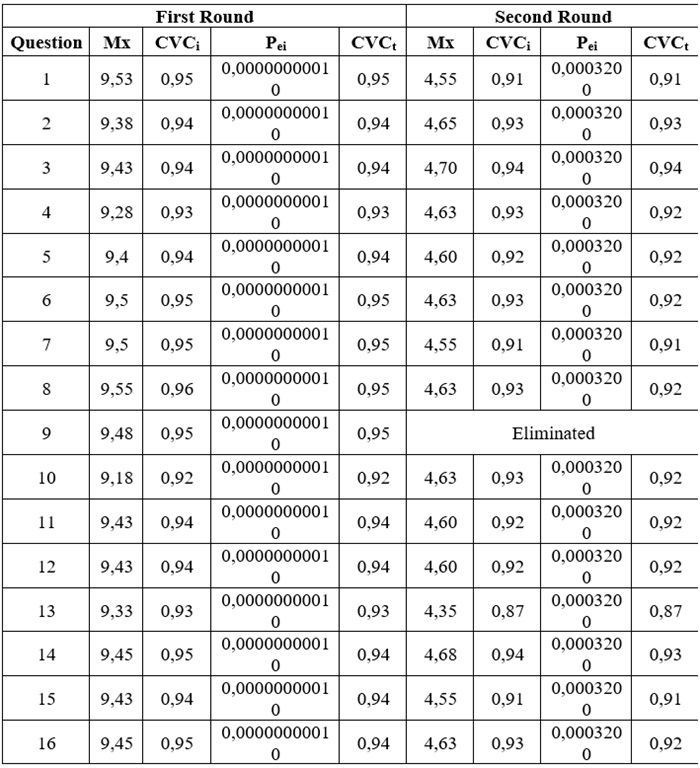
Six questions were removed from the questionnaire due to their complexity and redundancy, based on the experts' observations. These included items on the cleaning of the inner cannula, reinsertion after decannulation, and complications such as the tracheoesophageal fistula.
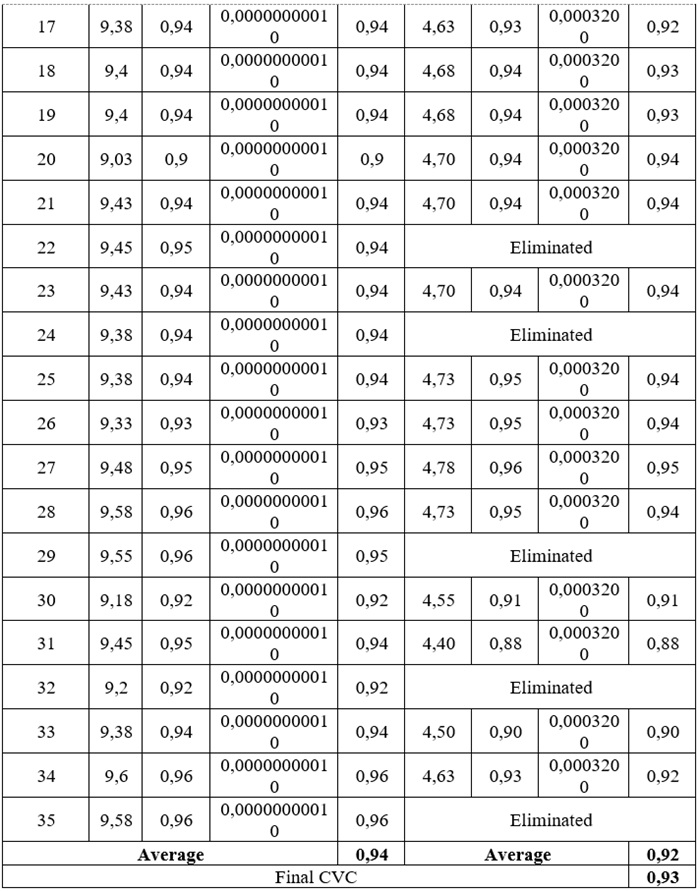
In the self-efficacy questionnaire, four items were removed due to redundancy or low relevance, according to the experts. These items addressed stoma care, respiratory observation, detection of complications, and materials management (Table 3).
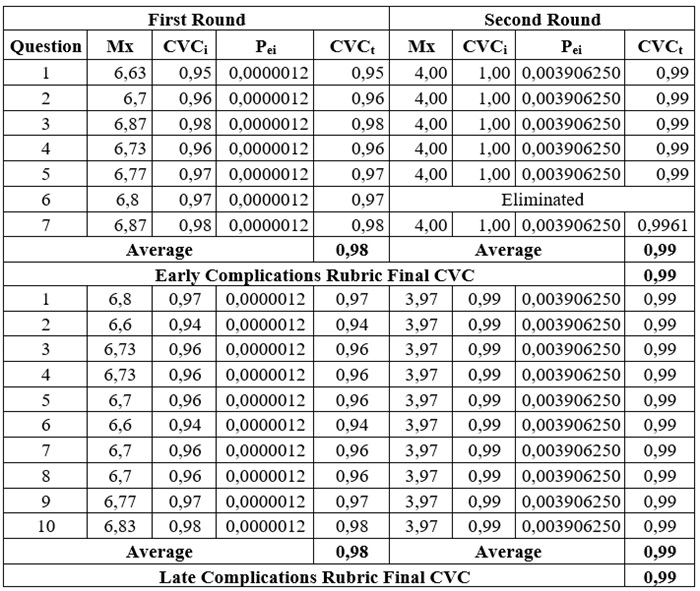
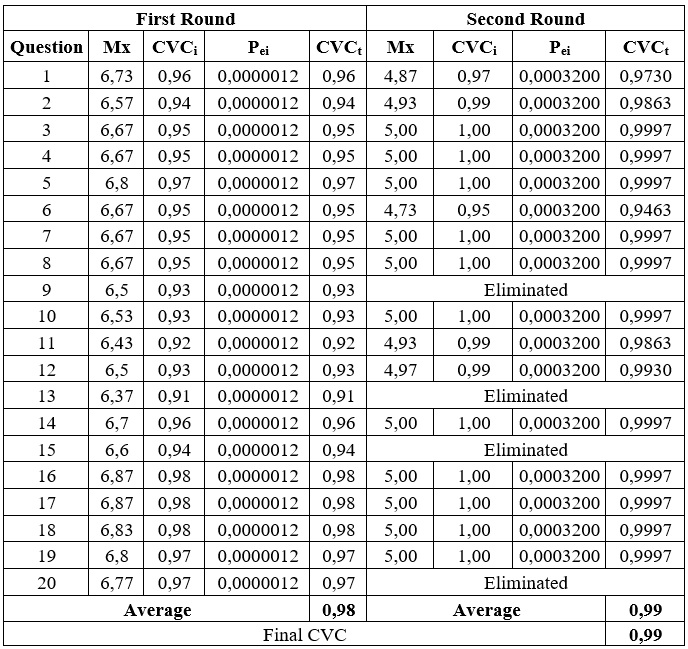
Regarding the Early Complications Identification Rubric, criterion 6 was removed as the experts identified it as repeated and redundant in relation to other evaluated criteria.
Both the questionnaires and the rubrics achieved CVC values greater than 0.90, surpassing the minimum cutoff of 0.80 set by Hernández-Nieto (18). Moreover, all items included in the final versions reached CVC values > 0.80, and the items eliminated were based on complexity, repetition, redundancy, or low relevance, as assessed by the experts.
Technical or ambiguous terms such as "most appropriate position," "accidental decannulation," or "stable patient" were identified as potentially unclear for family caregivers, and suggestions were made to replace them with more accessible expressions.
Additionally, questions with confusing wording or unclear sequences of actions were noted, such as those related to suction catheter use and securing the cannula. The experts also recommended clearer formulations. Furthermore, they advised specifying certain answers, such as the type of cloth or the use of hydrogen peroxide for cannula cleaning. All observations were considered, and necessary adjustments were made, improving the wording and adapting the content to the comprehension level of family caregivers, which strengthened both the questionnaires and rubrics.
Discussion
In the home care of patients with tracheostomies, it is crucial to have validated instruments to assess caregivers' knowledge and self-efficacy. The results from the design and validation of the two questionnaires and two rubrics show high content validity, supporting their usefulness for evaluating knowledge, self-efficacy, and complications in home tracheostomy management. Furthermore, they constitute valid tools for assessing preparation and confidence regarding complex procedures and emergencies, especially considering that many caregivers undertake these tasks without formal healthcare training (36-38).
The preparation of those involved in home tracheostomy management is vital, and this is supported by studies by Amar-Dolan et al. (5) and Yilmaz Yegit et al. (9), which have shown that structured caregiver training significantly improves their confidence and skills, thereby reducing adverse events such as infections and hospital readmissions. In this sense, the questionnaires from this study not only help identify educational deficiencies but also measure self-efficacy perception, offering a comprehensive view in training processes.
Regarding the clarity and relevance of the items, the adjustments made based on the experts' observations, particularly concerning technical language, reinforce the need to adapt the instruments to the target population defined for this study, i.e., family caregivers. This ensured that the items were understandable and relevant for their future application, as stated by Kasper et al. (39).
In adults with home tracheostomies, the most common complications include tube obstruction, displacement, infections, and device failures, with acute obstruction being a frequent emergency (13,40). Long-term complications, such as tracheal stenosis and tracheomalacia, may also arise (17). In this context, the inclusion of clinical rubrics provides more objective and structured assessment tools for recognizing complications. Having these rubrics facilitates the early (early complications) and late identification of adverse events, improving decision-making at home; it also serves as an evaluation tool that would support new interventions and contribute to safer care in the home setting.
The methodology used allowed the assessment of the CVC of the instruments through expert judgment in critical care, home care, and teaching. The main limitations include the absence of empirical validation with the target population and the limited size of the expert panel. Therefore, it is recommended to plan subsequent studies for construct validation, criterion validation, and reliability analysis through pilot tests with family caregivers .
Conclusions
This study allowed for the methodological design, refinement, and obtaining of the Content Validity Coefficient (CVC) through expert judgment for four instruments focused on the home care of adults with tracheostomies: two questionnaires (knowledge and self-efficacy) and two clinical rubrics for identifying early and late complications. As a result of the CVC process, the final versions of the instruments were consolidated, retaining only the items and clinical criteria with adequate clarity, relevance, and pertinence, supported by CVC values greater than 0.90.
References
1. Sherman J, Bower KL, Eskandanian K. “100 things I wish someone would have told me”: everyday challenges parents face while caring for their children with a tracheostomy. Qual Health Res. 2024 Sep 9;34(11):1108-18. https://doi.org/10.1177/10497323231217387
2. Chandran A, Sikka K, Thakar A, Lodha R, Irugu DVK, Kumar R, et al. The impact of pediatric tracheostomy on the quality of life of caregivers. Int J Pediatr Otorhinolaryngol. 2021; 149:110854. https://doi.org/10.1016/j.ijporl.2021.110854
3. Gong S, Wang X, Wang Y, Qu Y, Tang C, Yu Q, et al. A descriptive qualitative study of home care experiences in parents of children with tracheostomies. J Pediatr Nurs. 2019 Mar;45:7-12. https://doi.org/10.1016/j.pedn.2018.12.005
4. Mai K, Davis RK, Hamilton S, Robertson-James C, Calaman S, Turchi RM. Identifying caregiver needs for children with a tracheostomy living at home. Clin Pediatr (Phila). 2020 Nov 16;59(13):1169-81. https://doi.org/10.1177/0009922820941209
5. Amar-Dolan LG, Horn MH, O’Connell B, Parsons SK, Roussin CJ, Weinstock PH, et al. “This is how hard it is”: family experience of hospital-to-home transition with a tracheostomy. Ann Am Thorac Soc. 2020 Jul;17(7):860-8. https://doi.org/10.1513/AnnalsATS.201910-780OC
6. Şapulu Alakan Y, Akansel N, Özmen ÖA. Experiences of patients’ primary caregivers with tracheostomy suctioning before discharge. Eur J Oncol Nursing. 2023 Dec; 67:102435. https://doi.org/10.1016/j.ejon.2023.102435
7. Huestis MJ, Kahn CI, Tracy LF, Levi JR. Facebook group use among parents of children with tracheostomy. Otolaryngol Head Neck Surg. 2020 Mar 21;162(3):359-61. https://doi.org/10.1177/0194599820901528
8. Hall N, Rousseau N, Hamilton DW, Simpson AJ, Powell S, Brodlie M, et al. Providing care for children with tracheostomies: a qualitative interview study with parents and health professionals. BMJ Open. 2023 Jan 31;13(1):e065698. https://doi.org/10.1136/bmjopen-2022-065698
9. Yilmaz Yegit C, Kilinc AA, Can Oksay S, Unal F, Yazan H, Köstereli E, et al. The ISPAT project: implementation of a standardized training program for caregivers of children with tracheostomy. Pediatr Pulmonol. 2022 Jan 4;57(1):176-84. https://doi.org/10.1002/ppul.25704
10. Acorda DE, Jackson A, Lam AK, Molchen W. Overwhelmed to ownership: the lived experience of parents learning to become caregivers of children with tracheostomies. Int J Pediatr Otorhinolaryngol. 2022 Dec;163:111364. https://doi.org/10.1016/j.ijporl.2022.111364
11. Gaudreau PA, Greenlick H, Dong T, Levy M, Hackett A, Preciado D, et al. Preventing complications of pediatric tracheostomy through standardized wound care and parent education. JAMA Otolaryngol Head Neck Surg. 2016;142(10):966. https://doi.org/10.1001/jamaoto.2016.1803
12. Sterni LM, Collaco JM, Baker CD, Carroll JL, Sharma GD, Brozek JL, et al. An official American Thoracic Society Clinical Practice Guideline: pediatric chronic home invasive ventilation. Am J Respir Crit Care Med. 2016 Apr 15;193(8):e16-35. https://doi.org/10.1164/rccm.201602-0276ST
13. Mitchell RB, Hussey HM, Setzen G, Jacobs IN, Nussenbaum B, Dawson C, et al. Clinical Consensus Statement. Otolaryngol Head Neck Surg. 2013 Jan 18;148(1):6-20. https://doi.org/10.1177/0194599812460376
14. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191-215. https://doi.org/10.1037/0033-295X.84.2.191
15. Wang T, Voss JG, Schiltz N, Rezaee R, Chhabra N, Mazanec SR. Effectiveness of a pictorial educational brochure on tracheostomy care self-efficacy among patients with head and neck cancer and family caregivers: a quasi-experimental pilot study. Clin J Oncol Nurs. 2023;27(3):273-80. https://doi.org/10.1097/NCC.0000000000001237
16. Narwani V, Dacey S, Lerner MZ. Adverse events associated with tracheostomy: a MAUDE Database analysis. Otolaryngol Head Neck Surg. 2024 Feb 25;170(2):391-5. https://doi.org/10.1002/ohn.501
17. Zouk AN, Batra H. Managing complications of percutaneous tracheostomy and gastrostomy. J Thorac Dis. 2021 Aug;13(8):5314-30. https://doi.org/10.21037/jtd-19-3716
18. Hernández-Nieto RA. Contribuciones al análisis estadístico: coeficiente de validez de contenido. Mérida: Universidad de Los Andes; 2002.
19. Hernández Sampieri R, Fernández Collado C, Baptista Lucio MdelP. Metodología de la investigación [internet]. 6.ª ed. Madrid: McGraw-Hill-Interamericana; 2014 [citado 2025 mar 7]. Disponible en: http://repositorio.ucsh.cl/bitstream/handle/ucsh/2792/metodologia-de-la-investigacion.pdf?sequence=1
20. Kazi AM, Khalid W. Questionnaire designing and validation. J Pak Med Assoc. 2012 May;62(5):514-6. Disponible en: https://ecommons.aku.edu/pakistan_fhs_mc_women_childhealth_paediatr/14
21. Martín Arribas MC. Diseño y validación de cuestionarios. Matronas Profesión. 2004;5(17):23-9.
22. Care of adult patients in acute care facilities with a tracheostomy [internet]. Sydney: Agency for Clinical Innovation; 2021. Disponible en: https://aci.health.nsw.gov.au/networks/icnsw/clinicians/acute-tracheostomy
23. Agarwal A, Marks N, Wessel V, Willis D, Bai S, Tang X, et al. Improving knowledge, technical skills, and confidence among pediatric health care providers in the management of chronic tracheostomy using a simulation model. Pediatr Pulmonol. 2016;51(7):696-704. https://doi.org/10.1002/ppul.23355
24. Benjamin J, Roy K, Paul G, Kumar S, Charles E, Miller E, et al. Improving resident self-efficacy in tracheostomy management using a novel curriculum. MedEdPORTAL. 2020 Nov 3. https://doi.org/10.15766/mep_2374-8265.11010
25. Cordeiro ALP de C, Santos JAR e, Barroso ACL, Donoso MTV, Mata LRFP da, Chianca TCM. Tracheostomy care for adults and the elderly in the home environment: a scoping review. Rev Esc Enferm USP. 2024. https://doi.org/10.1590/1980-220x-reeusp-2024-0028en
26. Credland N. How to perform a tracheostomy dressing and inner cannula change. Nurs Stand. 2016 Mar 23;30(30):34-6. https://doi.org/10.7748/ns.30.30.34.s44
27. Flórez Pérez KA, Vargas Cortés MC, Manrique K, Soler Sierra AG, Puello Rico YL, Blanco Martínez AF, et al. Complicaciones tempranas de la traqueostomía en pacientes críticos. Ciencia Latina Rev Cient Multidisciplinar. 2024 Jul 23;8(4):40-54. https://doi.org/10.37811/cl_rcm.v8i4.12132
28. García MA, Barbero Peco C, Leoz Gordillo I, Garcia Salido A, Gaboli M. Traqueostomía y sus cuidados en pacientes pediátricos. Protoc Diagn Ter Pediatr. 2021;1:245-68.
29. Law C. Using mucociliary clearance methods that do not require an artificial airway. Nurs Times. 2003;99(41):57-9.
30. Organización Mundial de la Salud. Guía de la OMS sobre higiene de manos en la atención de la salud: resumen Primer Desafío Global de Seguridad del Paciente [internet]. 2009. Disponible en: https://www.who.int/publications/i/item/WHO_IER_PSP_2009.07
31. Queirós SMM, Pinto IES, de Brito MAC, Santos CSV de B. Nursing interventions for the promotion of tracheostomy self-care: a scoping review. J Clin Nurs. 2021 Nov 8;30(21-22):3055-71. https://doi.org/10.1111/jocn.15823
32. Smiths Medicals ASD. Manual de cuidados paciente adulto TQT Portex. 2008.
33. Texas Children’s Hospital. Manual para el cuidado del paciente con traqueostomía [internet]. Houston; 2021. Disponible en: https://www.texaschildrens.org/sites/default/files/uploads/documents/TrachBook_SPANISH_2021.pdf
34. Yelverton JC, Nguyen JH, Wan W, Kenerson MC, Schuman TA. Effectiveness of a standardized education process for tracheostomy care. Laryngoscope. 2015 Feb;125(2):342-7. https://doi.org/10.1002/lary.24821
35. Gatica-Lara F, Uribarren-Berrueta TdelNJ. ¿Cómo elaborar una rúbrica? Inv Ed Med. 2013;2(1):61-5. https://doi.org/10.1016/S2007-5057(13)72684-X
36. Amin R, Parshuram C, Kelso J, Lim A, Mateos D, Mitchell I, et al. Caregiver knowledge and skills to safely care for pediatric tracheostomy ventilation at home. Pediatr Pulmonol. 2017 Dec;52(12):1610-5. https://doi.org/10.1002/ppul.23842
37. McCoy JL, Williams KA, Senkinc JL, Westerman J, Tobey AB. Pediatric tracheostomy care simulation: real-life scenarios in a safe learning environment. Respir Care. 2022 Jan;67(1):40-7. https://doi.org/10.4187/respcare.09201
38. Prickett K, Deshpande A, Paschal H, Simon D, Hebbar KB. Simulation-based education to improve emergency management skills in caregivers of tracheostomy patients. Int J Pediatr Otorhinolaryngol. 2019 May;120:157-61. https://doi.org/10.1016/j.ijporl.2019.01.020
39. Kasper J, Lühnen J, Hinneburg J, Siebenhofer A, Posch N, Berger-Höger B, et al. MAPPinfo: mapping quality of health information: validation study of an assessment instrument. PLoS One. 2023 Oct 23;18(10):e0290027. https://doi.org/10.1371/journal.pone.0290027
40. Narwani V, Dacey S, Lerner MZ. Adverse events associated with tracheostomy: a MAUDE database analysis. Otolaryngol Head Neck Surg. 2024 Feb;170(2):391-5. https://doi.org/10.1002/ohn.501
Notes
Funding
It is declared that no
external funding was received for the development of this research.
Conflict of Interest
The authors declare that they have no conflict of
interest.
Author notes
a Correspondence author: edith.perianezl@uanl.edu.mx
Additional information
How to cite: Periañez López E, Moreno-Monsiváis MG.
Design
and Validation of Instruments to assess Knowledge, Self-efficacy, and
Complications in Home Tracheostomy Care. Univ Med. 2026;67. https://doi.org/10.11144/Javeriana.umed66.dvia
