








APA
ISO 690-2
Harvard
Haga clic en un formato de citación
In Vitro Determination of Working Length in Primary Teeth
Determinación in vitro de la longitud de trabajo en dientes primarios
Determinação in vitro do comprimento de trabalho em dentes decíduos
Maria Lorena Cardoso, Carlos Daniel Lugo de Langhe, Norma Griselda Díaz
In Vitro Determination of Working Length in Primary Teeth
Universitas Odontológica, vol. 41, 2022
Pontificia Universidad Javeriana
Maria Lorena Cardoso marialorenacardoso@hotmail.com
Universidad Nacional del Nordeste, Argentina
Carlos Daniel Lugo de Langhe lugocd@hotmail.com
Universidad Nacional del Nordest, Argentina
Norma Griselda Díaz normadiaz2089@gmail.com
Universidad Nacional del Nordeste, Argentina
Received: 18 march 2021
Accepted: 08 April 2022
Published: 31 october 2022
Abstract: Background: The success of a pulpectomy in temporary teeth depends on a precise execution of each one of the steps, such as the chemical-mechanical preparation. The requirement of the latter is to find the root canal’s real length, for which the direct method is the most accurate for in vitro measurements. Purpose: To determine in vitro the concordance of root lengths obtained from primary teeth using the radiographic method and the electronic apical locator (EAL). Methods: The study sample consisted of 40 primary molars extracted at the Pediatric Dentistry Clinic of the Universidad Nacional del Nordeste’s Dental School (Argentina), which met the experimental inclusion and exclusion criteria. The root canals were measured directly in vitro, by means of optical microscopy. Those findings were compared with measurements obtained radiographically and with EAL Results: The statistical analysis showed that the EAL coincided with the measurement obtained directly from the tooth in 79% of the cases. On the other hand, the coincidence between direct and radiographic measurements was only 52% (p=0.05). Conclusions: The use of EAL in primary molars can be useful to determine root length, which in turn would lead to better pulpectomy treatments and lower the risk of damage of permanent dental germs.
Keywords:dentistry, electronic apex locator, endodontics, pediatric dentistry, primary teeth, pulpectomy, root length.
Resumen: Antecedentes: El éxito del tratamiento de pulpectomía en dientes deciduos depende de una ejecución precisa de cada uno de los pasos, como la preparación químico-mecánica. Este último tiene como requisito hallar la longitud real del conducto radicular, para lo cual el método directo es el más exacto in vitro. Objetivo: Determinar in vitro la concordancia de la longitudes radiculares de dientes temporales obtenidas mediante el método radiográfico y el localizador apical electrónico (LAE). Métodos. La muestra del estudio consistió en 40 molares primarios extraídos en la Clínica de Odontopediatría de la Facultad de Odontología de la Universidad Nacional del Nordeste (Argentina), que cumplían con los criterios experimentales de inclusión y exclusión. Los conductos se midieron in vitro en forma directa, por medio de microscopia óptica. Esos hallazgos se compararon con las mediciones obtenidas radiográficamente y con LAE. Resultados: El análisis estadístico mostró que el LAE coincidió con la medida obtenida directamente del diente en un 80% de los casos. Por otra parte, la concordancia entre la medición directa y la radiográfica fue solo de un 52 % (p=0.05). Conclusiones: El uso de LAE en molares temporales puede ser útil para determinar la longitud de la raíz, lo que a su vez conduciría a mejores tratamientos de pulpectomía y disminuiría el riesgo de daño de los gérmenes dentales permanentes.
Palabras clave: dientes primarios, endodoncia, localizador apical electrónico, longitud radicular, odontología, odontología pediátrica, pulpectomía.
Resumo: Antecedentes: O sucesso do tratamento de pulpectomia em dentes decíduos depende da execução precisa de cada uma das etapas, como o preparo químico-mecânico. Este último é necessário para encontrar o comprimento real do canal radicular, para o qual o método direto é o mais preciso in vitro. Objetivo: Determinar in vitro a concordância dos comprimentos radiculares de dentes decíduos obtidos pelo método radiográfico e pelo localizador apical eletrônico (LAE). Métodos: A amostra do estudo foi composta por 40 molares decíduos extraídos na Clínica de Odontologia Pediátrica da Faculdade de Odontologia da Universidade Nacional do Nordeste (Argentina), que atenderam aos critérios experimentais de inclusão e exclusão. Os ductos foram medidos diretamente in vitro, por meio de microscopia de luz. Esses achados foram comparados com medidas obtidas radiograficamente e com LAE. Resultados: A análise estatística mostrou que o LAE coincidiu com a medida obtida diretamente do dente em 80 % dos casos. Por outro lado, a concordância entre as medidas diretas e radiográficas foi de apenas 52 % (p=0,05). Conclusões: O uso de LAE em molares decíduos pode ser útil na determinação do comprimento da raiz, o que, por sua vez, levaria a melhores tratamentos de pulpectomia e diminuiria o risco de danos por germes de dentes permanentes.
Palavras-chave: dentes decíduos, endodontia, localizador apical eletrônico, comprimento da raiz, odontologia, odontologia pediátrica, pulpectomia.
INTRODUCTION
The main goal of endodontic therapy in primary teeth is to preserve and maintain the integrity of the supporting structure when they present any condition that extends to the root pulp tissue. Thus, it is sought to remain until physiological exfoliation, preserving the length of the dental arch. The success of the pulpectomy treatment depends on an adequate execution of each of the steps, among which is the chemical-mechanical preparation.
An effective disinfection of the root canal consists of the complete elimination of necrotic pulp, microorganisms, and debris without affecting the periapical tissues and the follicle of the permanent tooth. Numerous reasons hinder the effective disinfection of these root canals in the primary dentition, such as the complex anatomical morphology of primary teeth, the continuous resorption process to which they are subjected, the proximity to the permanent successor, and the difficulty of producing satisfactory radiographic images of the apex due to their irregular rhizolysis (1). To minimize periapical lesions and possible damage to the permanent successor, root length should be carefully determined without exceeding the apices of the primary teeth at the time of canalometry (2). Therefore, the determination of the length of the roots is a crucial factor for the success of the endodontic treatment due to the importance of achieving complete disinfection of the canal without damaging the periapical tissues (3) and must also allow obtaining precise and reproducible results.
Conventional radiography and tactile sensation have been the techniques traditionally used to determine the working length in deciduous teeth. However, such methods may provide inaccurate information, imprecise lengths, and unreliable data, particularly in cases where physiological root resorption has begun (4,5). Conventional radiography in permanent teeth allows evaluating the radiographic image of the tooth with a file inserted into the dental canal up to 0.5 to 1.0 mm before the radiographic apex, a measure that corresponds to the anatomical apex. However, this measurement does not always coincide with the cement-dentinal junction (6,7). In primary teeth, the root working length using the radiographic technique is obtained by measuring, on the preoperative periapical radiograph with a millimeter ruler, the total size of the tooth (from an occlusal or incisal reference point to the root apex). Subsequently, 1-2 mm, preferably 2 mm, should be subtracted before the radiographic apex or rhizolysis bevel to obtain the actual working length (AWL) (8). The difficulties in obtaining the AWL through the radiographic study in these primary teeth are not only anatomical but are also related to the patient's cooperation and the limitation in mouth opening. These factors have stimulated the use of electronic devices for measuring the length of the root canal, which accurately report the foramen or more precisely an area between the smallest and largest diameter of the foramen.
The electronic apex locator (EAL) is an instrument that operates based on frequency, resistance, and impedance. EAL consists of a monitor that is attached by a cable, a lip hook, and a clip that connects to the file, closing the electrical circuit. Third generation EALs use multiple frequencies to determine the distance to the apical foramen but, like second generation EALs, measure impedance. To do this, they base their operation on the fact that the reactive component facilitates the flow of alternating current to a greater extent for higher frequencies. Thus, when two alternating currents pass through a tissue, the impedance will be higher in the lower frequency current. In this way, by measuring the impedance discrepancy between two frequencies and considering that the different points of the duct have a different impedance between high and low frequencies, a minimal difference is obtained in the coronal part of the canal. However, as the probe penetrates the duct, the difference increases and reaches its highest value at the height of the apical foramen, allowing it to be located more accurately (9).
Based on the benefits technology provides to optimize pulpectomy treatment, we considered important to know the performance of EAL devices in primary dentition and, although there are some studies that compare these three techniques in primary teeth (10-12), neither evaluates this difference of under- or over-instrumentation. The objective of our study was to determine the concordance between the root length obtained in vitro through the direct method, considering it as the AWL, and the measurements obtained with the radiographic method and the EAL in primary teeth.
MATERIALS AND METHODS
An experimental in vitro study was conducted with a sample of 40 primary teeth (13,14) that were extracted at the Pediatric Dentistry Clinic of the Universidad Nacional del Nordeste’s School of Dentistry (Argentina). Extraction of the teeth was indicated for any of the following reasons: prolonged retention (without spontaneous exfoliation), orthodontic purposes, or inability to restore adequately to ensure tooth permanence. The included teeth had to present a canal with more than two thirds complete and be permeable to the passage of a 10-K flexofile (Maillefer ®). Teeth with completely destroyed crowns and curved canals that prevented instrumentation were excluded.
Sample Preparation
The teeth, after extraction, were washed with a prophylactic brush and water and placed in 5.25 % sodium hypochlorite (Tedequim®), for two hours, to remove tissue remains. They were washed with running water and stored in distilled water until the time of the experiment. Teeth were numerically coded to allow control in data recording during AWL measurement with the different methods.
Experimental Procedures
The tooth samples were processed and measured by a single calibrated operator (Kappa = 0.9), who conducted the following procedure:
Cameral opening with round diamond bur No. 2 and thin truncated-cone bur.
Location of the canal with DG16 canal explorers (Maillefer®, Ballaigues, Switzerland).
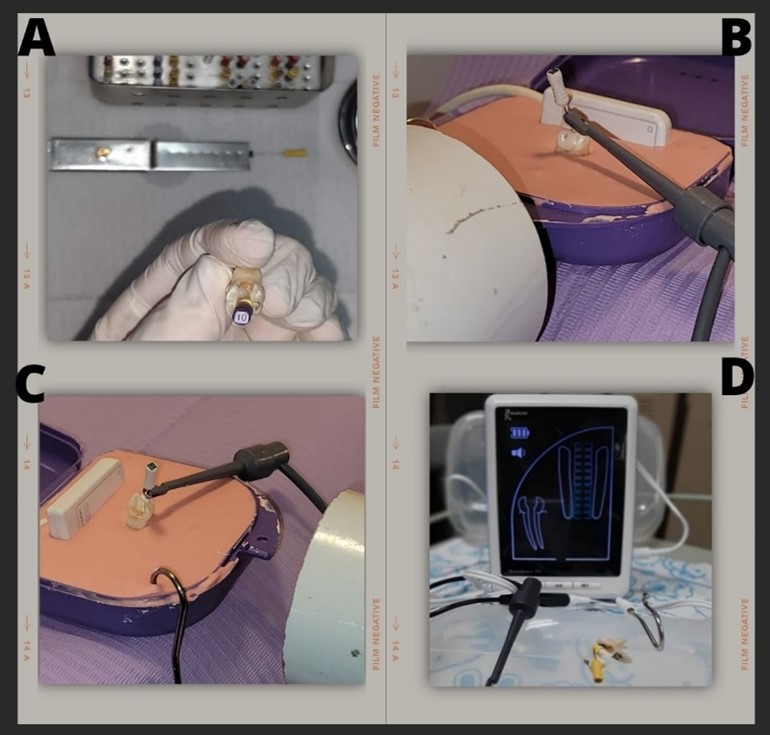
Catheterization of the root canals with #10 flexofile K-type files (Maillefer®, Ballaigues, Switzerland) to corroborate their permeability, determine and mark the dental canal to be measured (a single canal was measured from each tooth that met the inclusion and exclusion criteria) (Figure 1A).
A stable and fixed reference point was established for the rubber stop.
Once the canal was permeabilized and located, it was irrigated with 2.5 % sodium hypochlorite (Tedequim®), in order to provide a better movement of the instruments in the canal.
Measurement Techniques Used
Direct Method
In a first stage, the apices were observed under optical microscopy at 40x, identifying and recording the location of the foramen exits. The AWL was determined with K-type flexofile files (Maillefer®, Ballaigues, Switzerland), and then it was corroborated with optical microscopy that the files did not come out through the foramen. The length was fixed with the rubber stop, marking the reference coronal structure for taking the length. The files were measured with a millimeter ruler. To record the measurements with the EAL and the periapical radiographs, we used plastic boxes. Alginate (Orthoprint ®) was prepared according to the manufacturer's instructions and the containers were filled to position the teeth on the alginate.
Radiographic Method
The containers had a space for the alginate and a lateral slot for the radiographic sensor. This allowed to control the orthoradial and eccentric angulations during the taking of working length. The cone was placed at a distance of 5 cm from the objective in all cases (Figure 1B, 1C). On the image obtained through the Eagle Digital Sensor Image® program, the measurement was made from the reference point established for the direct method until the end of the root. 2 mm were subtracted from this value and the data was recorded in the survey forms.
AWL method
AWL was determined with the EAL Propex II® (Dentsply Maillefer) (Figure 1D). We made the measurements in triplicate for each sample in each experimental group.
Statistical Analysis
The recorded data were first analyzed descriptively and subsequently in triplicate with each of the techniques used; ANOVA was used to identify if there were significant differences and Tukey's test to determine exactly which data were significant. The software for the statistical analysis was Infostat 2021 (p < 0.05).
RESULTS
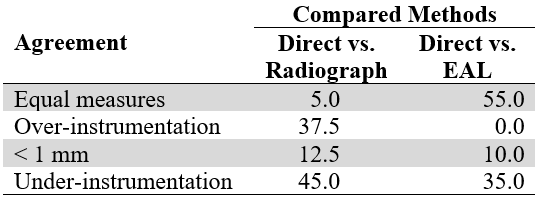
The sample consisted of 14 upper molars and 26 lower molars. The analysis of each tooth was first conducted by measuring by means of optical microscopy (direct method), establishing this reference as the AWL. Then, in triplicate, measurements were made with the radiographic method and the EAL, establishing the percentages of teeth that obtained a result equal to, higher (over-instrumentation), lower (~0.1-1 mm), or < 1 mm (under-instrumentation) than the AWL.
The radiographic method showed that the measurements in two teeth (5 %) agreed with the direct method. On the other hand, 57.5 % showed lower measurements, and 45 % (18 teeth) were under-instrumented. The remaining 12.5% had over-instrumentation. The comparison between the direct method and the EAL showed 55 % (22 teeth) of agreement with the direct method and 10 % with under-instrumentation of < 1 mm as part of 45 % of teeth with shorter AWL (table 1).
The measurements obtained from each tooth were compared in triplicate, establishing as a percentage how many measurements obtained coincided with those with the direct method. As can be seen in figure 2, 37.5% of the measurements did not show significant statistical differences between the three techniques and 42.5% of the measurements with EAL coincided with the RWL. In 15% of the cases, measurements with the direct and radiographic methods coincided (p = 0.05).
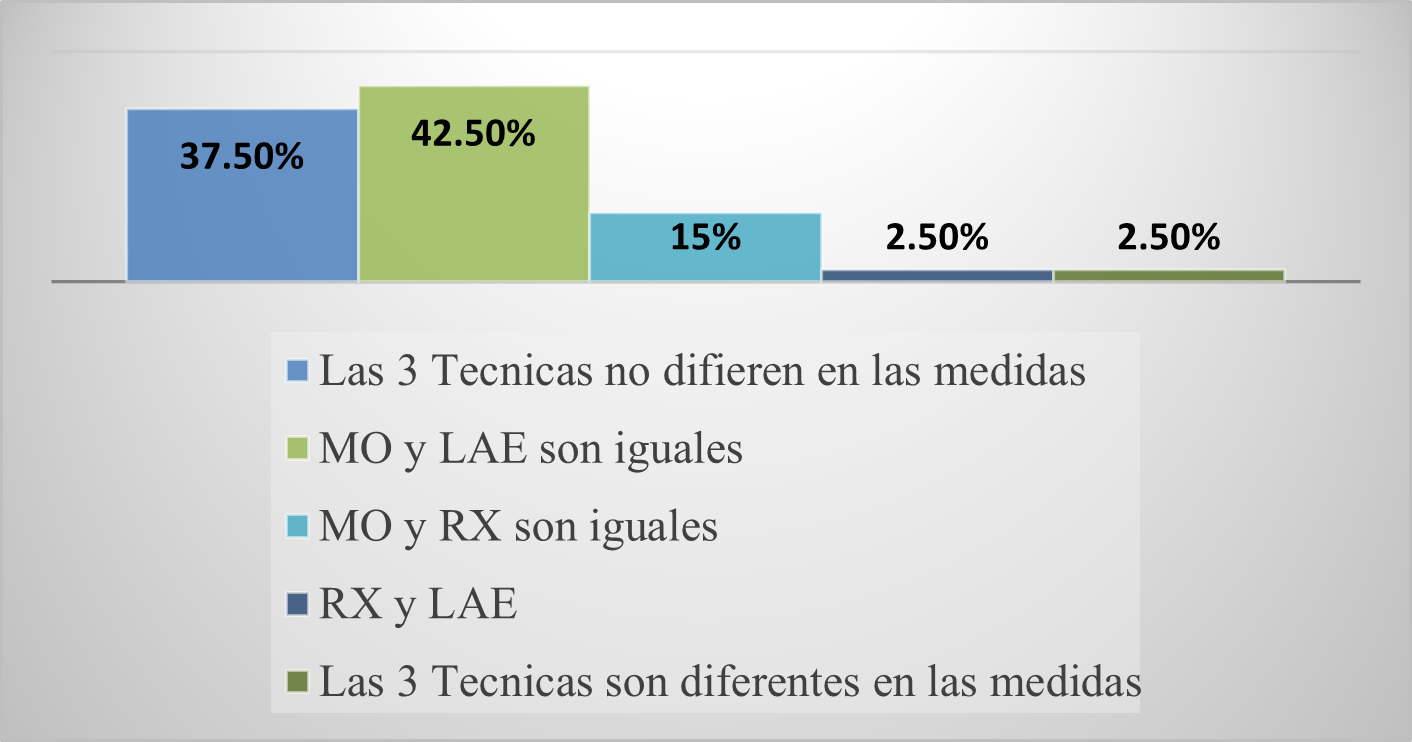
When the percentages of coincidence between the EAL and the direct method (42.5 %) and between the three methods (37.5 %) were added, it was obtained that in 80 % of the cases there was accuracy of the measurements with the electronic devices. The same analysis conducted with the radiographic method showed a coincidence of 52.5 % (p = 0.05).
DISCUSSION
The determination of the RWL in primary teeth is of the utmost importance to obtain a mechanical preparation and an effective obturation in treatments with pulpectomy, as well as being essential to avoid damage to the successor permanent teeth (15,16). The technique used to establish the length of the root canal must give accurate and reproducible results and, in many cases, tactile and conventional radiographic methods may be ineffective in this regard (17). The determination of the RWL is negatively affected by the anatomical variability of the root canal and the difficulty of visualizing these variations through radiographs. On the other hand, accurately positioning the file to establish a stable reference point requires a trained and standardized operator. To minimize such limitations, in the present study a single calibrated examiner performed all measurements.
Propex II is a modern fifth generation EAL using multi-frequency technology. Senthil, et al., (18) have used it in their studies and found that, in permanent teeth, it is better when compared with other EALs or with radiographic methods (18). Also, Propex II OS calculations are based on signal energy, while other apex locators typically use signal amplitude. Therefore, these authors also report that Propex II is less affected by possible interference in the root canal.
Thus, the present study only included primary molars (65% upper molars and 35% lower molars), which present greater difficulty in determining length, which has been reported by other studies (19). In the initial descriptive analysis, the individual measures with the radiographic method and the EAL were contrasted with the direct method. The findings revealed that the EAL had measurements equal to the direct method in 55% of the cases and values lower than the RWL in 45%. There were no cases of overextension. This is of great importance when seeking to preserve the successor tooth that is in close contact with the primary teeth. Over instrumentation or overfilling of primary teeth can damage the germ of the permanent successor (20).
On the other hand, when using the radiographic method, only 5 % of the measurements coincided with the RWL, 57.5 % had shorter lengths and 37.5 % had overextensions. These findings coincide with those of other authors for whom obtaining the RWL through the radiographic method was the least precise technique (21). These findings may be due to the way root length is established, overestimating what is real, due to the difficulty of determining the correct location of the apex, mainly due to the physiological resorption process that primary teeth undergo at different heights. Regarding the percentage of measurements that were shorter than the real one, that is, those that were < 1 mm were divided and highlighted, since this would not lead to effective disinfection or root filling in a system of canals as complex as those presented by these primary teeth ( 22).
As in this study, Topaloglu-Ak, et al. (12) used ex vivo primary molars, and performed three types of measurements: EAL through Propex II, digital radiography, and stereomicroscopy, to determine the actual length of the canals. These investigators found no statistically significant differences between the methods; however, their analysis only limited to looking at whether there was over-instrumentation or under-instrumentation (12).
In our statistical analysis, when adding the measures in which the three techniques established an equal RWL (37.5%) and the direct method and the LAE coincided (42.5%), we observed an 80% precision for the cases in which we used the RWL, exceeding the radiographic measurements that marked a 52.5% concordance (the 3 techniques averaged the same 37.5% plus 15%).
Supporting the evidence of this study, the use of EALs in primary molars can be a useful method to determine root lengths closer to reality and thus avoid over-instrumentation or under-instrumentation in pulpectomy treatments. Based on this research, projects will be started that estimate its usefulness in vivo to confirm whether its clinical application in temporary teeth is an optimal option in pulpectomy treatments.
References
1. Mente J, Seidel J, Buchalla W, Koch MJ. Electronic determination of root canal length in primary teeth with and without root resorption. Int Endod J. 2002. 35: 447-452. https://doi.org/10.1046/j.1365-2591.2002.00500.x
2. Holan G, Fuks AB. A comparison of pulpectomies using ZOE and KRI paste in primary molars: a retrospective study. Pediatr Dent. 1993 Nov-Dec; 15(6): 403-407.
3. Kielbassa AM, Muller U, Munz I, Monting JS. Clinical evaluation of the measuring accuracy of ROOT ZX in primary teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003 Jan;95(1):94-100. https://doi.org/10.1067/moe.2003.99
4. Subramaniam P, Konde S, Mandanna DK. An in vitro comparison of root canal measurement in primary teeth. J Indian Soc Pedod Prev Dent. 2005 Sep; 23(3): 124-125. https://doi.org/10.4103/0970-4388.16883
5. Bahrololoomi Z, Soleymani AA, Modaresi J, Imanian M, Lotfian M. Accuracy of an Electronic Apex Locator for working length determination in primary anterior teeth. J Dent (Tehran). 2015 Apr; 12(4): 243-248
6. Paludo L, Souza SL, Só MV, Rosa RA, Vier-Pelisser FV, Duarte MA. An in vivo radiographic evaluation of the accuracy of Apex and iPex electronic Apex locators. Braz Dent J. 2012; 23(1): 54-58. https://doi.org/10.1590/s0103-64402012000100010
7. Siu C, Marshall JG, Baumgartner JC. An in vivo comparison of the Root ZX II, the Apex NRG XFR, and Mini Apex Locator by using rotary nickel-titanium files. J Endod. 2009 Jul; 35(7): 962-965. https://doi.org/10.1016/j.joen.2009.04.025
8. Abanto J, Redua PCB, Bonecker M. Paso a paso para conductas clínicas en odontopediatria. Sao Paulo: Santos Publicaçoes 2020, 6: 105.
9. Baldi JV, Victorino FR, Bernardes RA, de Moraes IG, Bramante CM, Garcia RB, Bernardineli N. Influence of embedding media on the assessment of electronic apex locators. J Endod. 2007 Apr; 33(4): 476-479. https://doi.org/10.1016/j.joen.2006.12.024
10. Subramaniam P, Konde S, Mandanna DK. An in vitro comparison of root canal measurement in primary teeth. J Indian Soc Pedod Prev Dent. 2005 Sep; 23(3):124-125. https://doi.org/10.4103/0970-4388.16883
11. Bodur H, Odabaş M, Tulunoğlu O, Tinaz AC. Accuracy of two different apex locators in primary teeth with and without root resorption. Clin Oral Investig. 2008 Jun; 12(2): 137-141. https://doi.org/10.1007/s00784-007-0157-5
12. Topaloglu-Ak A, Aykut Yetkiner A, Güniz Baksi B, Eronat C. Ex vivo comparison of radiographic and electronic root canal length measurements in primary molars. Eur J Paediatr Dent. 2015 Jun; 16(2): 49-153.
13. Leonardo MR, Silva LA, Nelson-Filho P, Silva RA, Raffaini MS. Ex vivo evaluation of the accuracy of two electronic apex locators during root canal length determination in primary teeth. Int Endod J. 2008 Apr;41(4):317-21. https://doi.org/10.1111/j.1365-2591.2007.01366.x
14. Nelson-Filho P, Lucisano MP, Leonardo MR, da Silva RA, da Silva LA. Electronic working length determination in primary teeth by ProPex and digital signal processing. Aust Endod J. 2010 Dec; 36(3): 105-108. https://doi.org/10.1111/j.1747-4477.2009.00185.x
15. Ahmad IA, Pani SC. Accuracy of electronic apex locators in primary teeth: a meta-analysis. Int Endod J. 2015 Mar;48(3):298-307. https://doi.org/10.1111/iej.12315
16. Kumar LV, Sreelakshmi N, Reddy ER, Manjula M, Rani ST, Rajesh A. Clinical evaluation of conventional radiography, radiovisiography, and an electronic apex locator in determining the working length in primary teeth. Pediatr Dent. 2016 Jan-Feb;38(1):37-41
17. Govindaraju L, Jeevanandan G, Subramanian EMG. Comparison of quality of obturation and instrumentation time using hand files and two rotary file systems in primary molars: A single-blinded randomized controlled trial. Eur J Dent. 2017 Jul-Sep; 11(3): 376-379. https://doi.org/10.4103/ejd.ejd_345_16
18. Senthil D, Eagappan ARS, Sathivajeeva J, Ramkumar S, Srinivasan D, Loui J. Comparison of the accuracy of Propex II electronic apex locator and conventional radiography for working length determination in primary anterior teeth. J Int Oral Health. 2016. 8(6): 729-732. https://doi.org/10.2047/jioh-08-06-17
19. Toscano MA, Zacharczuk GA. Tratamiento con pasta 3Mix-MP en molares primarios no vitales: estudio preliminar. Bol Asoc Argent Odontol Niños. 2016; 44: 12-17.
20. Mente J, Seidel J, Buchalla W, Koch MJ. Electronic determination of root canal length in primary teeth with and without root resorption. Int Endod J. 2002 May; 35(5): 447-52. https://doi.org/10.1046/j.1365-2591.2002.00500.x
21. Abdullah A, Singh N, Rathore MS, Tandon S, Rajkumar B. Comparative evaluation of electronic apex locators and radiovisiography for working length determination in primary teeth in vivo. Int J Clin Pediatr Dent. 2016 Apr-Jun; 9(2): 118-123. https://doi.org/10.5005/jp-journals-10005-1346
22. Borges MMB, Guimarães BM, Alves JD, Sena GN, Bernardes NA, Duarte MAH. Evaluation of the accuracy of two apex locators in apical limit: an in vitro study. Rev Odontol Bras Central. 2016; 25(74):126-129.
Notes
*
Original research.
Author notes
Correspondence: marialorenacardoso@hotmail.com; mlcardoso@odn.unne.edu.ar; lugocd@hotmail.com; cdlugo@odn.unne.edu.ar; normadiaz2089@gmail.com
Additional information
How to cite this article: Cardoso ML, Lugo de Langhe CD, Diaz NG. In Vitro Determination of Working Length in Primary Teeth. Univ Odontol. 2022; 41. https://doi.org/10.11144/Javeriana.uo41.indw
