








APA
ISO 690-2
Harvard
Haga clic en un formato de citación
Assessment of Fears of the Covid-19 Pandemic in Spain *
Evaluación de los miedos ante la pandemia del COVID-19 en España
Aida Soriano ![]() , Aina Luque-García
, Aina Luque-García ![]() , Vicente Martínez-Tur
, Vicente Martínez-Tur ![]() , José M. Peiró
, José M. Peiró ![]()
Assessment of Fears of the Covid-19 Pandemic in Spain *
Universitas Psychologica, vol. 23, 2024
Pontificia Universidad Javeriana
Aida Soriano
Universitat de València, España
Aina Luque-García
Universidad Europea de Valencia, España
Vicente Martínez-Tur
Universitat de València, España
José M. Peiró a jose.m.peiro@uv.es
Universitat de València, España
Received: 16 august 2023
Accepted: 07 november 2024
Abstract: Due to the role that pandemic fears may play functionally and in terms of prevention, there is a need to monitor the changes and evolution of these fears. The present study aims to validate the revised Fear of Covid-19 Scale (FCS), which is used to measure Covid-19 fears, one year after the onset of the pandemic and the inception of the lockdown in Spain. Data were reported by 3 083 Spanish adults who answered the "Spaniards’ mental health during the COVID-19 pandemic Survey" of the Sociological Research Center (February 2021). Results of EFA, CFA (RMSEA = 0.052, CFI = 0.965, TLI = 0.955, and SRMR = 0.029), and other validity and reliability indices (e.g., Cronbach α ranged between 0.76 and 0.84) supported a four-factor solution: personal health-related fears, loved ones’ health-related fears, economic-employment-related fears, and social-related fears. Given the possibilities of having another crisis like the one created by Covid, it is important to have validated scales that can assess pandemic fears, due to the consequences these emotions can have for both individuals and society.
Keywords:Covid-19 fears, pandemic fears, FCS scale, Spanish validation, EFA, CFA.
Resumen: Debido al papel que los temores pandémicos pueden desempeñar funcionalmente y en términos de prevención, existe la necesidad de monitorear los cambios y la evolución de estos temores. El presente estudio tiene como objetivo validar la Escala Miedo de Covid-19 (FCS) revisada, que se utiliza para medir los miedos al Covid-19, un año después del inicio de la pandemia y del inicio del confinamiento en España. Los datos fueron aportados por 3 083 adultos españoles que respondieron la "Encuesta sobre la salud mental de los españoles durante la pandemia de COVID-19" del Centro de Investigaciones Sociológicas (febrero de 2021). Los resultados del AFE, AFC (RMSEA = 0.052, CFI = 0.965, TLI = 0.955 y SRMR = 0.029) y otros índices de validez y confiabilidad (e.g. alphas de Cronbach entre α = 0.76 y 0.84) respaldaron una solución de cuatro factores: miedos relacionados con la salud personal, miedos relacionados con la salud de sus seres queridos, miedos relacionados con la economía y el empleo, y miedos relacionados con la sociedad. Ante las posibilidades de tener otra crisis como la creada por el COVID, es importante contar con escalas validadas que puedan evaluar los temores pandémicos, por las consecuencias que estas emociones pueden tener tanto para los individuos como para la sociedad.
Palabras clave: miedos Covid-19, miedos pandemia, escala FCS, validación española, AFE, AFC.
COVID-19 reached Europe in January 2020. On March 14th, the Spanish Government, in a similar way to the rest of the governments of developed countries, decreed a state of alarm. This produced a disruptive alteration in the living conditions, productive and business activities, social relations, and work. Certain aspects of the disease were particularly ambiguous at the onset of the pandemic, such as uncertainty regarding the contagion process, its evolution, patient immunity, and the absence of a vaccine to combat the disease. These factors contributed to an increase in fear among the population (Luo et al., 2021; Rodríguez-Hidalgo et al., 2020). Initial reports indicated that contracting COVID-19 could be especially dangerous for certain risk groups, including the elderly and individuals with chronic illnesses (World Health Organization [WHO], 2021). This information suggested that people in these vulnerable groups would likely exhibit a stronger fear response due to their heightened risk of severe illness and mortality.
In general, fear has been and continues to be one of the most relevant psychological experiences, with clear health implications during the pandemic (Pakpour & Griffiths, 2020). Fear is a prototypical anticipatory negative emotion that is experienced in the present but based on the anticipation of a dangerous event in the future (Baumgartner et al., 2008). Although the investigation of future-oriented emotions has been relatively neglected (Seibel et al., 2020), living in fear is arguably one of the most detrimental experiences for overall well-being. In this context, COVID-19 not only impacts physical health but also contributes to various psychological disorders, significantly affecting the mental health of different communities (Salari et al., 2020; Fernández-Millán & Bretones, 2021). In this regard, there are several fearful conditions that emerged during the pandemics and should be identified. Recent empirical studies on the psychological impact of the COVID-19 pandemic report a wide range of fears associated with the coronavirus outbreak, highlighting the urgent need to address these issues in both clinical and public health settings. In this sense, several scales have been developed to assess Covid fears. Some measures aim to obtain a general Covid-19 fear score (Ahorsu et al., 2020; Mertens et al., 2020) and have been adapted to the Spanish population (Sánchez-Teruel et al., 2021), whereas others pay attention to its dimensions or facets (Sandín et al., 2020). For example, Coelho et al. (2020), in a review of 28 articles, identified the main types of Covid-19 fears studied: the unknown and uncertainty, social isolation, hypochondriasis, disgust, information-driven, and compliance. Additionally, some studies have qualitatively explored individuals’ fear concerns, identifying relevant facets such as their own contagion and health or the risk of loved ones getting the disease. Moreover, the fears were associated with the personal or family economy, due to a potential drop in income (e.g. losing one’s job/future prospects), and they were more broadly related to changes in the health system, the economy, the society, and daily routines and social life (Mertens et al., 2020).
Sandín et al. (2020) developed an 18-item scale (Fear of Covid-19 Scale[ FCS]), specifically designed within the Spanish context to assess fear in the general population during the lockdown period in Spain. They found that “the prevalence of these fears was very high, as more than 20 % of the population reported having experienced them with high or extreme intensity, and some fears appeared to be especially severe because they were felt very intensely by more than 40 % of participants. Among these fears are dread of the death of a close relative, infection of a close relative, spread of the virus, and isolation from close relatives and friends” (p. 12). Moreover, different types of fear presented specific relations with several vulnerability and protective factors, revealing the interest in considering different facets. A four-factor Covid-19 fear structure was found with the following factors: 1) fear of infection, disease, and death (personally or of a close relative); 2) fear of scarcity of basic consumer goods; 3) fear of social isolation; and 4) fears related to work and income.
In February 2021, the Spanish Center for Sociological Studies (CIS) launched the "Spaniards’ Mental Health during the COVID-19 Pandemic Survey", specifically aimed at understanding fears within the Spanish context. This survey used an adapted version of the FCS, modified to better reflect concerns in Spain’s evolving situation. Some items were excluded (e.g. food or other essential products becoming scarce), probably because they might be relevant during the lockdown period but were not anymore in the different context studied in the CIS survey in February 2021. Furthermore, two new items were added to the scale: one about changes in society, and the other about pandemics becoming part of our lives.
Considering the existence of a previous structured proposal for a measure of fear of Covid (Sandín et al., 2020) and the changes implemented by the CIS to adapt to the changing reality of the health crisis caused by COVID, there is a need to validate whether this factorial structure is still valid. Therefore, this study aims to validate the revised FCS scale that was used to measure Covid-19 fears one year after the onset of the pandemic and the inception of the lockdown in Spain. In order to do so, we will obtain the factor structure and other validity and reliability indexes for the revised scale. Examining the nature and quality of the FCS will make it possible to better track people’s fears, not only in relation to Covid-19, but also in other possible health crises that may arise in the future, as an indicator of how a given crisis is affecting the wellbeing of individuals and the community as a whole.
Method
Sample and Procedure
The sample used for the present study was composed of 3 083 adults from 1 080 Spanish municipalities and 50 provinces. These data come from the "Spaniards’ mental health during the COVID-19 pandemic Survey" (Centro de Investigaciones Sociológicas [CIS], 2021), which took place in February 2021 through a computer-assisted telephone interview. Phone numbers were randomly selected, including both landline (27.3 %) and mobile (72.7 %) contacts. Additionally, sex and age quotas were applied to select the participants. Forty-nine per cent of the sample were men, and the participants ranged in age from 18 to 98 years old (M = 50.82; SD = 16.82).
As previously said, the data used in this study were obtained from the CIS, which adheres to a strict Ethical Code and Good Practice Guidelines (Centro de Investigaciones Sociológicas [CIS], 2021) to ensure the confidentiality and anonymity of participants. The CIS Ethical Code emphasizes principles of impartiality, respect for the Constitution of Spain, legal order, and fundamental rights. It ensures that research is conducted with objectivity, transparency, and effectiveness, while adhering to laws and safeguarding public rights and freedoms. The code promotes ethical and professional responsibility in public management and scientific research, grounded in values such as transparency and rigor. For more details, you can refer to the full document https://www.cis.es/documents/d/cis/codigo_etico.
Measures
The "Spaniards’ mental health during the COVID-19 pandemic Survey" assessed behaviors, experiences, effects, and consequences of the COVID-19 pandemic. For the present research, we specifically focused on pandemic fears and other variables of interest such as sociodemographic data and negative affect.
Pandemic fears were measured with a 15-item scale. These items assessed the degree to which an individual has experienced COVID-19-related fears from the beginning of the pandemic until now. The original response scale ranged from 1 (very much) to 5 (not at all). However, to facilitate result interpretation and maintain consistency with other scales where higher scores indicate greater intensity of the measured construct, the response scale was inverted in the present investigation. The inverted scale is as follows: 1 (not at all; originally 5) - 5 (very much; originally 1). This inversion allows higher scores to represent higher levels of COVID-19-related fear, which is more intuitive and aligns with other measures used in the study. All data analyses were conducted using these inverted values, ensuring that calculations and results accurately reflect the direction of scale where 5 represents the maximum level of fear.
Sex. The response scale ranged from 1 (man) to 2 (woman).
Age. Participants indicated their age. Then, different categories were created to allow comparisons between groups: 1) 30 years old or less; 2) between 31 and 50 years old; 3) between 51 and 64 years old; 4) 65 years old or more.
Living with people with chronic illness. The response scale ranged from 1 (yes) to 2 (no).
Employment situation. Participants indicated their employment situation, which was categorized as: 1) Employed; 2) Retired/pensioner; 3) Unemployed; 4) Student; 5) unpaid domestic work.
Educational level. Participants indicated their employment situation, which was categorized as: 1) Without studies, 2) Elementary studies, 3) Compulsory secondary school or equivalent, 4) Upper Vocational and educational training and voluntary secondary school, 5) Bachelor’s degree studies, 6) Postgrad studies, and 7) PhD degree.
Social class. Participants indicated their employment situation, and this information was categorized as: 1) Lower class 2) Middle-lower class, 3) Middle class, and 4) Upper or middle-upper class.Having been infected by COVID-19. The response scale ranged from 1 (yes) to 2 (no).
Whether a close family member has been infected by COVID-19. The response scale ranged from 1 (yes) to 2 (no).
Whether a close family member has died from COVID-19. The response scale ranged from 1 (yes) to 2 (no).
Negative affect was measured with a 4-item scale (sample item: “during the pandemic period, how frequently have you felt down, depressed, or hopeless”). The response scale ranged from 1 (A lot of days) to 4 (Never). The response scale was inverted to analyze the data from the present investigation to facilitate the reader's understanding (thus, 1 = never-; 4 = a lot of days). The Cronbach’s . for the scale was 0.81.
Data Analysis
First, descriptive statistics were computed using SPSS v.26 (IBM Corp., 2019) to assess the data distribution’s normality. The kurtosis and skewness values (between -2 and +2) guaranteed the assumptions of normality, supporting the use of parametric tests for the subsequent analyses (Hair et al., 2010).
Second, reliability was examined with the Cronbach’s alpha value and McDonald’s coefficient omega, which are the most widely used measures of composite reliability (Zhang & Yuan, 2015). Hair et al. (2010) state that a value of 0.70 is generally agreed upon as an acceptable value for Cronbach’s alpha, whereas for the omega value, coefficients should exceed 0.50 as a minimum, but 0.75 would be preferred (Reise, 2012; Reise et al., 2013).
Third, Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) were carried out to analyze whether the items followed the hypothesized factor structure proposed by the authors. Thus, a cross-validation was conducted by applying EFA to one half of the sample (randomly) and CFA to the other half (Brown, 2006). This double analysis allows us to achieve more solid results if consistency is observed between them. Considering the characteristics of the sample, for the CFA, the ML method and PROMIN oblique rotation were used (Ferrando & Anguiano-Carrasco, 2010; Kiers, 1994; Lorenzo-Seva, 1999). Additionally, based on this cross-validation, a CFA was also performed with the whole sample using MPLUS software (Muthén & Muthén, 1998-2017). In order to assess the fit of the model, we examined the RMSEA (Root Mean Square Error Approximation), CFI (Comparative Fit Index), TLI (Tucker-Lewis Index), and SRMR (Root Mean Square Residual) goodness of fit statistics. Cutoff values of less than 0.06 for RMSEA, more than 0.95 for CFI and TLI, and less than 0.08 for SRMR typically reflect an optimal fit to the data (Hu & Bentler, 2009; Little, 2013).
Finally, discriminant and convergent validity were tested with a t-test for dichotomous variables, ANOVA for variables with three or more response options, and Pearson correlations for continuous variables.
Results
Most common pandemic fears associated with COVID-19
To examine the most common pandemic fears associated with COVID-19, we computed the percentage of participants who experienced each fear (e.g. items) quite or very intensely.
First, it is worth mentioning that not all the pandemic fears considered induced the same degree of fear in the participants. The three items with the greatest impact were: “that coronavirus continues to spread” (75.9 % of participants indicated that they experienced this fear quite or very intensely); “that a family member or loved one could die” (72.5 %); and “that a family member or loved one could catch it” (68.9 %). These results are quite similar to those obtained by Sandín et al. (2020), given that these items were also the ones with the highest level of fear (although the highest one was “that a family member or loved one could catch it” instead of “that coronavirus continues to spread”).
Furthermore, items that were in the top 10 COVID-19-related fears in the Sandín et al. (2020) study have now lost a bit of prominence. These items refer to fear of losing employment or income. Nevertheless, aspects that were not considered in previous studies are currently in the top 10 COVID-related fears: “that society will never be the same as before” and “that pandemics will become part of our life”.
Finally, the fears that participants experienced less were “dying from coronavirus” (23.6 %) and “being alone or socially isolated” (33.5 %). In this case, the situation was very different from Sandín et al. (2020) study because the items that had less impact in their study were not included in the current research: “that food or other essential products become scarce” and “that you could be left without important things in the house”.
The comparison of the scores of groups of men and women separately showed that all the pandemic fears have a significantly greater impact on women than on men. Additionally, when comparing different age ranges, significant differences were found between groups on all the items except the fear “that a family member or loved one would lose his/her job” and “that pandemics will become part of our life”. In this regard, the oldest group of participants (65 years old and up) had the least pandemic fear (on all the items with significant differences), except on the item about the fear “that something serious would happen to you (an accident, an illness, etc.) and you’d have to go to the emergency room”, where older participants showed more fear than the other groups.
Internal consistency
Reliability
Table 1 reports means, standard deviations, correlations, Cronbach’s alphas, and omega values for each factor of the pandemic fears scale. Cronbach’s alphas and omega scores ranged between 0.76 and 0.84, indicating excellent reliability.

Factor structure
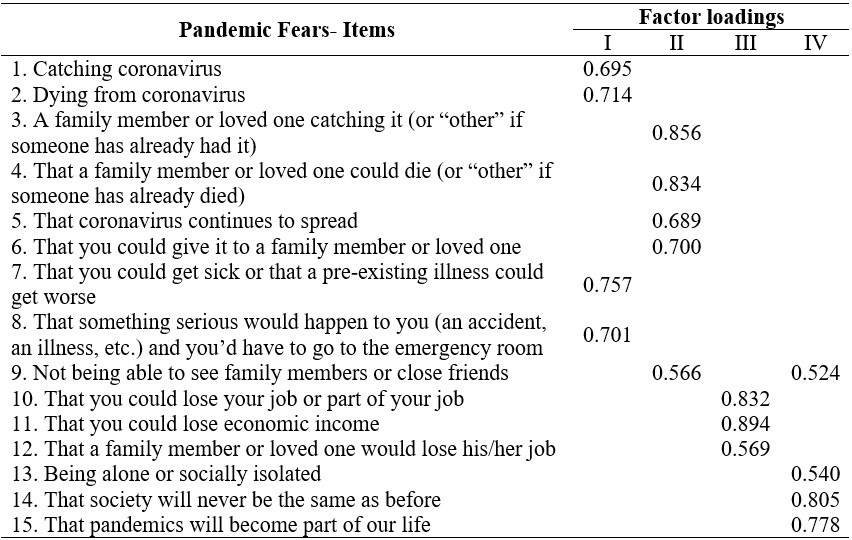
First, EFA was applied to one half of the sample. The two criteria to identify the number of factors on the scales were: Cattell eigenvalues greater than the point of change of the slope in the sedimentation curve and Kaiser’s eigenvalues higher than 1. According to both Kaiser’s and Cattell’s criteria, the EFA yielded a four-factor solution. Second, a CFA was applied to the other half of the sample. Table 2 shows factor loadings after oblique rotation. Four factors were obtained: 1) personal health-related fear, 2) loved ones’ health-related fear, 3) economic/employment-related fear, and 4) social-related fear. Note that Item 9 “not being able to see family members or close friends”, loads on two factors, Factors II and IV. Because both loadings are higher than 0.40 (Hair et al., 1998) and considering previous evidence that includes this item as part of the social factor (Sandín et al., 2020), we have also considered it a social-related fear.
Additionally, we also tested a CFA considering the whole sample in order to assess the fit of the model using MPLUS software. Results showed that the internal structure suggested by our previous analyses had an acceptable fit: RMSEA = 0.079, CFI = 0.916, TLI = 0.895, and SRMR = 0.063. To confirm that Item 9 belongs to social-related fear, we compared the fit of our model to another model, including it as part of factor II. Adding support to previous evidence, the fit of our model is better than when this item is considered in the loved ones’ health-related fear factor (RMSEA = 0.093, CFI = 0.883, TLI = 0.854, and SRMR = 0.085).
Considering the large correlations among the four dimensions of the model (Table 1), a one-factor model might be more suitable to represent pandemic fear. To evaluate this possibility, we compared the four-factor model with a single-factor model specifying that all indicators would load onto one general factor. The results showed that the four-factor model fits the data better than the alternative one-factor solution (RMSEA = 0.131, CFI = 0.752, TLI = 0.711, and SRMR = 0.079). Furthermore, after examining parameter estimates, fit indexes, and residuals, we made modifications to the original hypothesized model to achieve a better fitting and more parsimonious model. MPLUS software calculated modification indexes, which suggested correlating the residuals of some items within the same factor. These modifications were carefully considered based on both statistical and theoretical grounds. Specifically, we correlated the residuals of Items 3 and 4 (Factor II), as they likely share common variance due to their similar content related to fears about loved ones' health; Items 10 and 11 (Factor III), which both address economic concerns and capture a specific aspect of financial fear; and Items 14 and 15 (Factor IV), focusing on society-related fears that may share unique variance related to the impact of pandemics on society. These correlations were allowed only between items within the same factor to maintain the overall integrity of the factor structure. After implementing these theoretically justifiable modifications, the model showed an excellent fit (RMSEA = 0.052, CFI = 0.965, TLI = 0.955, and SRMR = 0.029), improving our understanding of the interrelationships between items while preserving the conceptual four-factor structure.
Discriminant and Convergent Validity
The different factors of the pandemic fears scale were analyzed considering sociodemographic data of interest. First, results of T tests showed that: 1) women present higher levels of fear in all factors (p < 0.05) than men; 2) participants who live with people with chronic illness have higher levels of fear in all factors (p < 0.05) than participants who do not; 3) individuals who have a close family member who has been infected with COVID-19 present higher levels of loved ones’ health-related fear and social-related fear (p < 0.05); and 4) participants who have a family member who died from COVID-19 have higher levels of personal health-related fear, loved ones’ health-related fear, and social-related fear (p < 0.05) than participants who do not. No significant differences in any of the pandemic fear factors were found between individuals who have been infected by COVID-19 and participants who have not.
Second, results of ANOVA tests showed differences in pandemic fears between groups based on their age, employment situation, educational level, and social class. In the case of age, results show that, generally, the older the participant, the less the pandemic fear. The older group (65 years old or more) showed less loved ones’ health-related fear, economic/employment-related fear, and social-related fear than the other groups (p < 0.05). Moreover, the older group showed less personal health-related fear than the participants whose ages ranged between 31 and 64 years old (p < 0.05). Additionally, participants from 51-64 years old showed less loved ones’ health-related fear and economic/employment fear than the younger groups (p < 0.05).
Regarding the educational level, results indicated that participants with higher vocational and educational training and non-compulsory secondary school presented more loved ones’ health-related fear than participants with elementary studies (p< 0.05). Additionally, the higher the educational level, the lower the economic/employment fear (the PhD degree group presented less fear than the other groups; the postgrad studies group showed less fear than participants with compulsory secondary school or the equivalent, and individuals with bachelor’s degree studies presented less fear than those with compulsory secondary school or the equivalent and upper vocational and educational training and non-compulsory secondary school; p < 0.05).
With regard to the employment situation, unemployed participants showed higher levels of personal health-related fears than employed participants (p < 0.05), and employed and unpaid domestic workers presented more fear than retired/pensioner participants (p < 0.05). Moreover, retired/pensioner participants showed less loved ones’ health-related fear and economic/employment-related fear than the other groups (p < 0.05), and unemployed participants presented higher levels of economic/employment-related fear than the other groups (p < 0.05). Additionally, regarding social-related fear, retired/pensioner individuals presented less fear than the employed and unemployed groups, and employed participants showed less fear than unemployed ones (p < 0.05).
Regarding the social class, the lower-class group showed more personal health-related fear than the other groups (p < 0.05), and the middle-class group also presented more fear than the upper or middle upper-class group (p < 0.05). Additionally, the lower-class group showed more loved ones’ health-related fear than the upper or middle upper-class group (p < 0.05). Finally, in the case of the other two pandemic fear factors, results showed that the higher the social class, the lower the economic/employment and social-related fears (p < 0.05).
The different factors of the pandemic fears scale were correlated with the negative affect scale. Scores on negative affect were positively correlated with all these dimensions of pandemic fear: personal health-related fear (r = 0.39; p < 0.05), loved ones’-related health fear (r = 0.36; p < 0.05), economic/employment-related fear (r = 0.28; p < 0.05), and social-related fear (r= 0.42; p < 0.05), thus indicating convergent validity.
Discussion
The objective of this research was to validate the revised FCS scale, which was used by the CIS to measure Covid-19 fears one year after the beginning of the lockdown in Spain and the onset of the pandemic. To do so, we obtained the factor structure and other validity and reliability indexes for the revised scale.
Several studies in the reviewed literature have evaluated Covid-19 fear. Some studies have applied a single-item methodology (e.g. Sánchez-Teruel et al., 2021), whereas other studies, like ours, have paid attention to the different dimensions or facets of fear (e.g. Mertens et al., 2020; Sandín et al., 2020). Accordingly, results of the present research show that the four-factor model fits the data better than a one-factor alternative solution. These four factors refer to: 1) personal health-related fear, 2) loved ones' health-related fear, 3) economic/employment-related fear, and 4) social-related fear.
Regarding the item analyses, the three items that showed a higher level of impact were: “that coronavirus continues to spread”, “that a family member or loved one could die”, and “that a family member or loved one could catch it”. These results coincide with those obtained by Sandín et al. (2020). However, elements that refer to the fear of losing one’s job and/or income have lost some prominence, and aspects that were not considered by these authors (e.g. that society will never be the same as before) are now in the current top 10 of COVID-related fears. Accordingly, it is important to highlight the changing nature of the pandemic in terms of the experience of different types of fear. There is evidence of a change in the fears linked to the different situations that occurred during the pandemic (the fears are different depending on whether we are locked down at home or on the street with masks in the middle of a wave, etc.).
Likewise, our results showed differences in pandemic fears between the different sociodemographic variables in relation to the four factors analyzed. First, the results showed, in general, that the older the participant, the lower the fear of the pandemic. This intriguing finding could be attributed to several factors. One possible explanation is that older individuals may have developed greater resilience over time, having faced and overcome various life challenges, including previous health crises. Their life experience might provide them with a broader perspective on adversity, potentially reducing anxiety about current threats. Another hypothesis is that older individuals might perceive the pandemic differently due to their life stage; they may have a more accepting attitude towards health risks. Conversely, younger individuals might experience higher levels of fear due to greater uncertainty about their future plans and career prospects in light of the pandemic's economic impact. Furthermore, the pervasive use of social media among younger generations could contribute to heightened anxiety through constant exposure to pandemic-related information and news.
The data also showed that participants who live with people with chronic illnesses have higher levels of fear across all factors than participants who do not. Moreover, people who have a close relative who has been infected with COVID-19 present higher levels of fear related to the health of loved ones and social fear. These data are supported by the literature, given that contagion, and even the fear of one’s own death or that of a loved one, was, at that time, a real possibility when living with COVID-19 patients, with repetitive thoughts of rumination focused on the past being more likely (Sánchez-Teruel et al., 2021). In fact, data have been published on people who live with patients with COVID-19, and these people may have a greater predisposition to developing depression (Huang et al., 2020). Furthermore, and as might be expected, our data also showed that participants who have a family member who died from COVID-19 presented higher levels of fear related to personal health, fear related to the health of loved ones, and social fear, compared to the participants who do not have one (Cao et al., 2020).
Regarding the educational level, results indicated that participants with professional training and non-compulsory higher and secondary education presented more fear related to the health of loved ones than participants with elementary studies (Cerda & García, 2022). In addition, a higher educational level implied less economic/labor fear. This could be explained by the fact that having a higher educational level could be associated with financial stability, which acts as a protective factor against anxiety (Cao et al., 2020).
With regard to the employment situation, the unemployed participants showed higher levels of fear related to personal health, compared to the employed participants, and employed individuals and unpaid domestic workers presented more fear than retired/pensioner participants. Additionally, the retired/pensioner participants showed less fear related to the health of loved ones and economic/work fear than the other groups. These results are consistent with what has been described in the literature (Adams et al., 2012; Sandín et al., 2020) and could indicate that older age could be a protective factor against fear and concern about the coronavirus and its consequences.
Regarding the social class, the results showed that the higher the social class, the lower the economic/labor and social fears. The lower social class group showed more personal fear related to health than the other groups, and the middle-class group also presented more fear than the high or middle-high class group. Likewise, differences between sexes were also found. All the pandemic fears have a significantly greater impact on women than on men. These data are consistent with the evidence found in the literature, and they suggest a greater vulnerability of women to suffering from fears and phobias, regardless of the type of fear in question (Adams et al., 2012; Sandín et al., 2020).
This study presents some limitations that open the door to new elaborations and approaches to the subject. One of them is related to the cross-sectional nature of the study, which significantly limits the inferences drawn about the results. Because of this, we are unable to investigate issues of directionality or causality in the data, meaning that our results only inform us about a specific moment and certain circumstances. Another limitation of the study is that the data used belong to a representative Spanish sample. Although this sample allows us to obtain relevant and significant data, we cannot generalize beyond this country because the data are not universal. As stated in a previous study (Peiró et al., 2023), although fear is a universal emotion, its experience may vary depending on the cultural framework (Ali et al., 2021). Finally, our study focuses on the prototypical future-oriented negative emotion: fear. This choice is reasonable, considering the problems caused by the pandemic; however, considering the prototypical positive future-oriented emotion (hope) (Baumgartner et al., 2008) could provide complementary insights. For example, it would be useful to study whether hope for positive changes during the pandemic (such as a more compassionate society) could enhance positive affect and reduce somatic problems. Future studies should examine these variables in this new context of COVID-19. Additionally, it would be beneficial to conduct longitudinal studies to address these limitations and gain a deeper understanding of how these feelings evolve over time, as well as to include samples from different countries to facilitate cross-cultural comparisons.
Furthermore, it should be mentioned that, since March 2020, and more specifically in the past year, there have been important changes in the knowledge, information, and effectiveness of vaccines and treatments for Covid-19. All of this has had an impact on the perception of the disease itself, the risks it entails, the social significance as stigma, and the fears that Covid-19 produces. Before we had effective vaccines or treatments, avoiding transmission was of great importance, but the emergence of new Covid-19 variables, along with the discovery of new vaccines and treatments, caused significant changes in the way of approaching the situation at a social and sanitary level. In fact, the recovery of social life and the progressive normalization in the different spheres of social relations (in the educational, work, recreational fields, etc.) are confirmed. However, Covid-19 has not yet been eradicated, which presents new challenges because there are patients with persistent sequelae (respiratory disorders, nervous system disorders, etc.), and we must also be aware of the appearance of new strains that may be more aggressive and future waves. Another important issue is that the number of emerging infectious diseases increased significantly in the second half of the 20th century, most of them zoonotic in nature and originating in wildlife. Among the determinants associated with the emergence of these diseases are human interactions with ecosystems, loss of biodiversity, changes in land use, climate change, trade and consumption of wildlife, etc. (Sánchez et al., 2022). Therefore, current societies are prone to facing other pandemics that generate fear, like Covid-19.
The findings from the present research have relevant practical implications related to knowledge, management of fears, and the consequences of these fears. As mentioned in the previous work by Peiró et al. (2023), fears can be functional because they warn the person about possible problems; however, fears are dysfunctional if they become negative obsessive thoughts that cause psychological distress and somatization. Given that the risk of suffering future pandemics is high, it is important to have validated scales like ours that can assess the consequences of the different Covid fears for individuals and for society. In fact, previous evidence suggests that these dimensions of Covid fear have consequences for people, knowledge, and fear management.
Additionally, these results have practical implications not only for the intervention of mental health professionals but also for the involvement of other relevant professionals, such as doctors and social workers, who have direct contact with and influence on various population groups. For instance, mental health professionals can utilize the FCS scale to assess and address the specific fears and anxieties experienced by their clients, tailoring interventions accordingly. Similarly, doctors can implement the scale in clinical settings to identify patients who may be experiencing heightened pandemic-related fears, allowing for timely support and resources. Social workers can also apply the scale to understand the emotional well-being of individuals in their care, enabling them to provide appropriate support and connect them with necessary resources. By integrating the FCS scale into these diverse professional practices, we can enhance the overall response to mental health needs during public health crises and better support vulnerable populations. Likewise, on a social level, the media and social networks play a crucial role, given that they can exaggerate bad news, creating exaggerated fears in the population (Lin, 2020). Along these lines, previous reports show that greater exposure to the media is related to the manifestation of greater fear (Garfin et al., 2020; Van den Bulck & Custers, 2009). Taking these results into account, providing information without sensationalism or disturbing images would have a great impact on the population (Garfin et al., 2020). Therefore, it is important for the media, governments, authorities, and civil society to organize a communication system that provides accurate information about crises, avoiding unnecessary fear. This practice, based on evidence, could also be promoted in different contexts (universities, companies, public administrations, schools, NGOs, etc.). Additionally, people could be advised to somewhat restrict their exposure to media coverage of the COVID-19 crisis (for example, verify media sources only a limited number of times a day and not continuously throughout the day) and avoid sensationalist media that can increase stress and decrease wellbeing. In sum, informative actions and action strategies should be designed by public and private institutions with competences in the different areas involved in health and social wellbeing to ensure a correct perception by the population of the risks and characteristics of pandemics and their implications for economic and social activities.
Conclusion
There is still certain ambiguity about the future evolution of the pandemic, even in a context of gradual normalization of social life. Its evolution presents new circumstances that may have an impact on the intensity, functions, and facets of the fears of Covid-19. In this study, the revised FCS scale was used to measure fears of Covid-19 one year after the start of the pandemic and the confinement in Spain, and it has been validated. For this purpose, the factorial structure and other indices of validity and reliability of the revised scale have been studied.
There is a need to monitor the changes and evolution of pandemic fears at an individual and collective level, given that they can play both functional and preventive roles and even hinder people's health and wellbeing. Therefore, it is important to highlight the central role of the revised FCS in assessing pandemic fears and their consequences.
References
Adams, T. G., Sawchuk, C. N., Cisler, J. M., Lohr, J. M., & Olalunji, B. O. (2012). Specific phobias. In P. Emmelkamp y T. Ehring (Eds.). The Wiley handbook of anxiety disorders (vol. 1, pp. 297-320). Chichester, UK: Wiley. https://doi.org/10.1002/9781118775349.ch18
Ahorsu, D. K., Lin, C. -Y., Imani, V., Saffari, M., Griffiths, M.D., & Pakpour, A. H. (2020). The fear of COVID-19 scale: development and initial validation. International Journal of Mental Health and Addiction, 20, 1537-1545. https://doi.org/10.1007/s11469-020-00270-8
Ali, M., Uddin, Z., Banik, P. C., Hegazy, F. A., Zaman, S., Ambia, A. S. M., Siddique, K. B., Islam, R., Khanam, F., Bahalul, S. M., Sharker, M. A., Hossain, F., & Ahsan, G. U. (2021). Knowledge, attitude, practice, and fear of COVID-19: An online-based cross-cultural study. International Journal of Mental Health and Addiction, 21, 1025 - 1040. https://doi.org/10.1007/s11469-021-00638-4
Baumgartner, H., Pieters, R., & Bagozzi, R. P. (2008). Future-oriented emotions: Conceptualization and behavioral effects. European Journal of Social Psychology, 38(4), 685–696. https://doi.org/10.1002/ejsp.467
Brown, T.A. (2006). Confirmatory factor analysis for applied research. 1th ed.; Guilford Press: New York.
Cao, W., Fang, Z., Hou, G., Han, M., Xu, X., Dong, J., & Zheng, J. (2020). The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Research, 287, 112934. https://doi.org/10.1016/j.psychres.2020.112934
Centro de Investigaciones Sociológicas [CIS]. (2021). Código ético y de buenas prácticas. Ministerio de la Presidencia, relaciones con las cortes y memoria democrática: Spain. https://www.cis.es/documents/d/cis/codigo_etico
Centro de Investigaciones Sociológicas [CIS] (2021). Encuesta sobre la salud mental de los/as españoles/as durante la pandemia de la COVID-19. Spain. https://consaludmental.org/centro-documentacion/encuesta-salud-mental-covid19-cis/
Cerda, A. A., & García, L.Y. (2022). Factors explaining the fear of being infected with COVID-19. Health Expectations, 25(2), 506– 512. https://doi.org/10.1111/hex.13274
Coelho, C. M., Suttiwan, P., Arato, N., & Zsido, A. N. (2020) On the nature of fear and anxiety triggered by COVID-19. Frontiers in Psychololy. 11, 581314. https://doi.org/10.3389/fpsyg.2020.581314
Ferrando, P. J., & Anguiano-Carrasco, C. (2010). El análisis factorial como técnica de investigación en psicología. Papeles del psicólogo, 31(1), 18-33. https://www.redalyc.org/pdf/778/77812441003.pdf
Fernández-Millán, J. M., & Bretones, F. D. (2021). Salud mental y factores de resiliencia durante el confinamiento por COVID-19. Universitas Psychologica, 19, 1–13. https://doi.org/10.11144/Javeriana.upsy19.smfr
Garfin, D. R., Silver, R. C., & Holman, E. A. (2020). The novel coronavirus (COVID-2019) outbreak: Amplification of public health consequences by media exposure. Health Psychology, 39(5), 355-357. https://doi.org/10.1037/hea0000875
Hair, J. F., Anderson, R. E., Tatham, R. L. & Black, W. C. (1998). Multivariate data analysis with readings (5th ed.). Upper Saddle River, NJ: Prentice-Hall.
Hair, J. F., Black, W. C., Babin, B. J., & Anderson, R. E. (2010). Multivariate Data Analysis: International Version, 7th ed.; Pearson Education: Saddle River, NJ, USA. https://www.drnishikantjha.com/papersCollection/Multivariate%20Data%20Analysis.pdf
Hu, L. -T., & Bentler, P. M. (2009). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural equation modeling: a multidisciplinary journal, 6(1), 1-55. https://doi.org/10.1080/10705519909540118
Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., Zhang, L., Fan, G., Xu, J., Gu, X., Cheng, Z., Yu, T., Xia, J., Wei, Y., Wu, W., Xie, X., Yin, W., Li, H., Liu, M., . . . Cao, B. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet, 395(10223), 497–506. https://doi.org/10.1016/S0140-6736(20)30183-5
IBM Corp. (2019). IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp.
Kiers, H. A. (1994). Simplimax: Oblique rotation to an optimal target with simple structure. Psychometrika, 59(4), 567-579. https://doi.org/10.1007/BF02294392
Lin, C. -Y. (2020). Social reaction toward the 2019 novel coronavirus (COVID-19). Social Health and Behavior, 3(1), 1–2. https://doi.org/10.4103/SHB.SHB_11_20
Little, T. D. (2013). Longitudinal structural equation modeling. 1th ed. Guilford press: New York.
Lorenzo-Seva, U. (1999.). Promin: A method for oblique factor rotation. Multivariate behavioral research, 34(3), 347-365. https://doi.org/10.1207/S15327906MBR3403_3
Luo, F., Gheshlagh, R. G., Dalvand, S., Saedmoucheshi, S., & Li, Q. (2021). Systematic review and meta-analysis of fear of COVID-19. Frontiers in psychology, 12, 661078. https://doi.org/10.3389/fpsyg.2021.661078
Mertens, G., Gerritsen, L., Duijndam, S., Salemink, E., & Engelhard, I. M. (2020). Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. Journal of anxiety disorders, 74, 102258. https://doi.org/10.1016/j.janxdis.2020.102258
Muthén, L. K., & Muthén, B. O. (1998-2017). Mplus User's Guide. Eight Edition. Los Angeles, CA: Muthén & Muthén.
Peiró, J. M., Luque-García, A., Soriano, A., & Martínez-Tur, V. (2023). Fears during the Covid-19 pandemics and their influence on physical health: A cross-sectional study on the general population in Spain. International journal of clinical and health psychology, 23(2), 100361. https://doi.org/10.1016/j.ijchp.2022.100361
Pakpour, A. H., & Griffiths, M. D. (2020). The fear of COVID-19 and its role in preventive behaviors. Journal of Concurrent Disorders, 2(1), 58-63. https://doi.org/10.54127/WCIC8036
Reise, S. P. (2012). The rediscovery of bifactor measurement models. Multivariate Behavioral Research, 47(5), 667–696. https://doi.org/10.1080/00273171.2012.715555
Reise, S. P., Bonifay, W. E., & Haviland, M. G. (2013). Scoring and modeling psychological measures in the presence of multidimensionality. Journal of Personality Assessment, 95(2), 129–140. https://doi.org/10.1080/00223891.2012.725437
Rodríguez-Hidalgo, A. J., Pantaleón, Y., Dios, I., & Falla, D. (2020). Fear of COVID-19, stress, and anxiety in university undergraduate students: a predictive model for depression. Frontiers in psychology, 11, 591797. https://doi.org/10.3389/fpsyg.2020.591797
Salari, N., Hosseinian-Far, A., Jalali, R., Vaisi-Raygani, A., Rasoulpoor, S., Mohammadi, M., Rasoulpoor, S., & Khaledi-Paveh, B. (2020). Prevalence of Stress, Anxiety, Depression among the General Population during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Globalization and Health, 16(57), 1-11. https://doi.org/10.1186/s12992-020-00589-w
Sánchez, A., Contreras, A., Corrales, J. C., & de la Fe, C. (2022). En el principio fue la zoonosis: One Health para combatir esta y futuras pandemias. Informe SESPAS 2022 [In the beginning it was zoonosis: One Health to combat this and future pandemics. SESPAS Report 2022]. Gaceta sanitaria, 36(1), S61–S67. https://doi.org/10.1016/j.gaceta.2022.01.012
Sánchez-Teruel, D., Robles-Bello, M. A., & Valencia-Naranjo, N. (2021). Do psychological strengths protect college students confined by COVID-19 to emotional distress? The role of gender. Personality and Individual Differences, 171, 110507. https://doi.org/10.1016/j.paid.2020.110507
Sandín, B., Valiente, R. M., García-Escalera, J., & Chorot, P. (2020). Impacto psicológico de la pandemia de COVID-19: Efectos negativos y positivos en población española asociados al periodo de confinamiento nacional. Revista de Psicopatología y Psicología Clínica, 25(1), 1-22. https://doi.org/10.5944/rppc.27569
Santabárbara, J., Bueno-Notivol, J., Lipnicki, D. M., Olaya, B., Pérez-Moreno, M., Gracia-García, P., Idoiaga-Mondragon, N. & Ozamiz-Etxebarria, N. (2021). Prevalence of anxiety in health care professionals during the COVID-19 pandemic: A rapid systematic review (on published articles in Medline) with meta-analysis. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 107, 110244. https://doi.org/10.1016/j.pnpbp.2021.110244
Seibel, S., Volmer, J., & Syrek, C. J. (2020). Get a taste of your leisure time: The relationship between leisure thoughts, pleasant anticipation, and work engagement. European Journal of Work and Organizational Psychology, 29(6), 889–906. https://doi.org/10.1080/1359432X.2020.1804875
Van den Bulck, J., & Custers, K. (2009). Television exposure is related to fear of avian flu, an Ecological Study across 23 member states of the European Union. European Journal of Public Health, 19(4), 370–374. https://doi.org/10.1093/eurpub/ckp061
World Health Organization [WHO]. (2021). WHO COVID-19 dashboard. https://covid19.who.int/
World Health Organization [WHO]. (2020). WHO COVID-19 preparedness and response progress report-1 February to 30 June 2020. https://www.who.int/publications/m/item/who-covid-19-preparedness-and-response-progress-report---1-february-to-30-june-2020
Zhang, Z., & Yuan, K. -H. (2015). Robust coefficients alpha and omega and confidence intervals with outlying observations and missing data: Methods and software. Educational and Psychological Measurement, 76(3), 387-411. https://doi.org/10.1177/0013164415594658
Notes
*
Research
article. The authors declare that no funding was
received from any entity for this study. There are no conflicts of interest to
disclose. No AI tools were used to generate any sections of this document.
Author notes
aCorrespondence author. Email: jose.m.peiro@uv.es
Additional information
How to cite: Soriano, A., Luque-García,
A., Martínez-Tur, V., & Peiró, J. M. (2024). Assessment
of Fears of the Covid-19 Pandemic in Spain. Universitas
Psychologica, 23, 1-14. https://doi.org/10.11144/Javeriana.upsy23.afcp
